
2023 , Vol. 20 >Issue 02: 207 - 212
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.02.009
超声心动图对非瓣膜性心房颤动患者左心房及左心耳功能的评价及血栓形成预测因素分析
Copy editor: 汪荣
收稿日期: 2021-08-28
网络出版日期: 2023-05-22
版权
Evaluation of left atrium and left atrial appendage function and risk factors for thrombosis in patients with non-valvular atrial fibrillation by echocardiography
Received date: 2021-08-28
Online published: 2023-05-22
Copyright
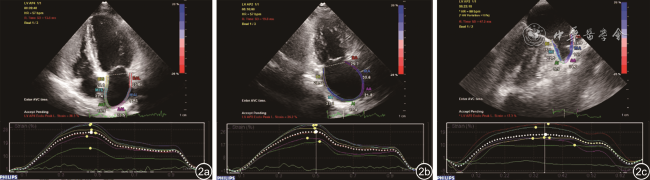
应用二维经胸超声心动图(TTE)、经食管超声心动图(TEE)及斑点追踪技术(STE)评价非瓣膜性心房颤动(NVAF)患者左心房及左心耳功能,并探讨其对左心房及左心耳血栓形成的预测价值。
选取2019年9月至2021年6月辽宁省人民医院的NVAF患者101例,根据TEE的结果将患者分为血栓组(47例)和非血栓组(54例)。采集患者的临床基本信息及N-末端脑钠肽前体(NT-proBNP)。TTE基本参数测量:左心房前后径(LAD)、左心室前后径(LVD)、室间隔厚度(IVS)、左心室后壁厚度(LVPW)、左心室射血分数(LVEF)、左心室舒张末期容积(LVEDV)。左心房功能参数:左心房最大容积指数(LAVImax)、左心房最小容积指数(LAVImin)、左心房射血分数(LAEF)、左心房峰值纵向应变(LA PLS)。TEE测量左心耳排空速度(LAAEV)、左心耳口直径(LAAD)、左心耳深度(LAAL)、左心耳最大容积(LAAVmax)、左心耳最小容积(LAAVmin)、左心耳射血分数(LAAEF)、左心耳峰值纵向应变(LAA PLS)及左心耳形态,并比较2组患者的临床特征及超声心动图参数。将有统计学意义的参数纳入多因素Logistic回归,分析左心耳血栓形成的预测因素并绘制ROC曲线分析预测价值。
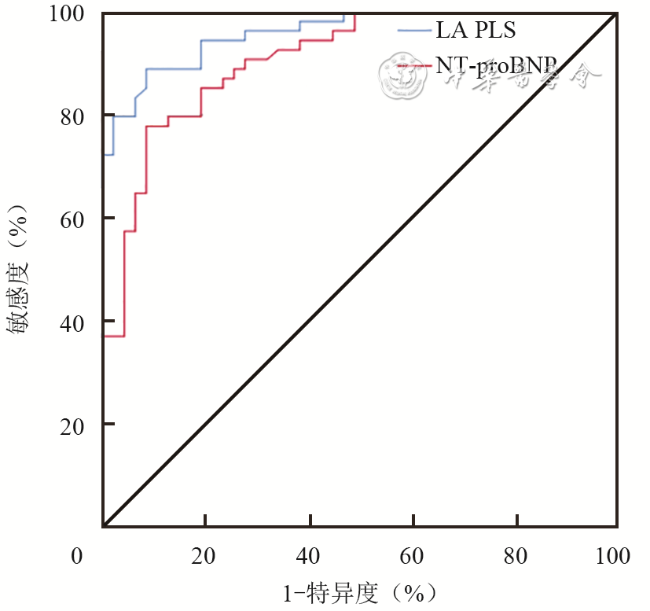
单因素分析结果显示,与非血栓组相比,血栓组患者持续性心房颤动发生率、NT-proBNP、LAD、LAVImax、LAVImin、LAAVmax、LAAVmin均显著升高,LAEF、LA PLS,LAAEV、LAAEF、LAA PLS显著降低(P均<0.05)。多因素Logistic回归分析显示,BNP(OR值:1.003;95%CI:1.000~1.007;P=0.045)和LA PLS(OR值:0.668;95%CI:0.515~0.920;P=0.012)是预测左心耳血栓的独立危险因素。ROC曲线分析结果显示,NT-proBNP的最佳截断值为243.2 pg/ml(曲线下面积为0.909,敏感度为91.5%,特异度为77.8%,准确性84.2%),LA PLS的最佳截断值15.75%(曲线下面积为0.960,敏感度为88.9%,特异度为91.5%,准确性90.1%)。
超声心动图可有效评价心房颤动患者左心房和左心耳的结构和功能,NT-proBNP和LA PLS与NVAF患者左心房及左心耳血栓具有独立相关关系,其有助于临床医师识别血栓形成风险相对较高的患者。
郑雨萌 , 丁明岩 , 孙丹丹 , 郭丽娟 , 张慧慧 , 赵含章 , 朱芳 . 超声心动图对非瓣膜性心房颤动患者左心房及左心耳功能的评价及血栓形成预测因素分析[J]. 中华医学超声杂志(电子版), 2023 , 20(02) : 207 -212 . DOI: 10.3877/cma.j.issn.1672-6448.2023.02.009
To evaluate the function of the left atrium and left atrial appendage and identify the independent risk factors for left atrial and left atrial appendage thrombosis in non-valvular atrial fibrillation (NVAF) patients using transthoracic echocardiography (TTE), transesophageal echocardiography (TEE), and speckle tracking echocardiography (STE).
This study included 101 consecutive NVAF patients who underwent TEE at the People's Hospital of Liaoning Province. The patients were divided into two groups based on the presence of left atrium and left atrial appendage thrombosis or not: 47 patients (46.5%) with left atrium and left atrial appendage thrombosis and 54 patients (54.5%) without. TTE, TEE, and STE were performed to assess the function of the left atrium and left atrial appendage. The clinical characteristics, N-terminal proBNP (NT-proBNP), echocardiography parameters, and left atrial appendage morphology were compared between the two groups. Multivariate regression analysis was performed to to identify predictive factors for left atrial appendage thrombosis. ROC curve analysis was performed to calculate the diagnostic efficacy of the predictive factors for thrombosis.
The prevalence of persistent atrial fibrillation, NT-proBNP, left atrial anteroposterior diameter, left atrial maximum volume index, left atrial minimum volume index, and left atrial appendage maximal volume and minimal volume in the thrombosis group were significantly higher than those in the non-thrombosis group. Left atrial ejection fraction, left ventricle ejection fraction, left atrial appendage emptying velocity, left atrial appendage ejection fraction, left atrial peak longitudinal strain (LA PLS) and left atrial appendage peak longitudinal strain (LAA PLS) in the thrombosis group were lower than those of the non-thrombosis group. Multivariate logistic regression analysis revealed that NT-proBNP (odds ratio [OR]=1.003; 95% confidence interval [CI]: 1.000~1.007, P=0.045) and LA PLS (OR=0.668, 95%CI: 0.515~0.920, P=0.012) were the independent risk factor for left atrium and left atrial appendage thrombosis (P<0.05). The cut-off values for NT-proBNP and LA PLS for predicting the presence of left atrium and left atrial appendage thrombosis were 243.2 pg/ml (AUC=0.909, sensitivity 91.5%, specificity 77.8%, accuracy 84.2%) and 15.75% (AUC=0.960, sensitivity 88.9%, specificity 91.5%, accuracy 90.1%), respectively.
Echocardiography can effectively evaluate the structure and function of the left atrium and left atrial appendage in patients with NVAF. NT-proBNP and LA PLS are independently associated with the thrombosis of the left atrium and left atrial appendage in patients with NVAF, which can help clinicians to identify patients at a relatively high risk of thrombosis.
表1 血栓组与非血栓组患者的一般资料比较 |
| 临床资料 | 血栓组(n=47) | 非血栓组(n=54) | P值 |
|---|---|---|---|
| 年龄(岁, | 62.9±10.39 | 58.6±11.44 | 0.052 |
| 身高(cm, | 168.96±8.27 | 167.44±7.96 | 0.352 |
| 体重(kg, | 75.67±14.70 | 73.88±12.71 | 0.513 |
| BMI(kg/m2, | 26.32±3.92 | 26.34±3.63 | 0.916 |
| BSA(m2, | 1.85±0.22 | 1.81±0.20 | 0.450 |
| 男性[例(%)] | 32(68.1) | 27(50.0) | 0.066 |
| 吸烟[例(%)] | 16(34.0) | 13(24.1) | 0.269 |
| 饮酒[例(%)] | 17(36.2) | 11(20.4) | 0.077 |
| 冠心病[例(%)] | 11(23.4) | 12(22.2) | 0.841 |
| 糖尿病[例(%)] | 8(17.0) | 5(9.3) | 0.245 |
| 高血压[例(%)] | 27(57.4) | 22(40.7) | 0.094 |
| 持续性心房颤动[例(%)] | 38(80.9) | 8(14.8) | <0.001 |
| NT-proBNP[pg/ml,M(QR)] | 826(134.3) | 144(165.2) | <0.001 |
注:BMI为体质量指数;BSA为体表面积;NT-proBNP为N-末端脑钠肽前体 |
表2 血栓组与非血栓组超声心动图基本参数比较( |
| 参数 | 血栓组(n=47) | 非血栓组(n=54) | P值 |
|---|---|---|---|
| LVD(mm) | 47.68±4.04 | 46.35±3.19 | 0.068 |
| IVS(mm) | 10.87±1.42 | 10.96±1.69 | 0.773 |
| LVPW(mm) | 10.57±1.43 | 10.22±1.65 | 0.256 |
| LVEDV(ml) | 98.32±19.16 | 91.7±15.05 | 0.055 |
| LVEF[%,M(QR)] | 0.55(0.04) | 0.57(0.05) | <0.001 |
注:LVD为左心室前后径;IVS为室间隔厚度;LVPW为左心室后壁厚度;LVEDV为左心室舒张末期容积;LVEF为左心室射血分数 |
表3 血栓组与非血栓组左心房功能参数比较( |
| 参数 | 血栓组(n=47) | 非血栓组(n=54) | P值 |
|---|---|---|---|
| LAD(mm) | 44.49±4.05 | 40.00±3.91 | <0.001 |
| LAVImax(ml/m2) | 43.68±10.05 | 35.01±7.22 | <0.001 |
| LAVImin(ml/m2) | 33.03±8.69 | 21.50±4.94 | <0.001 |
| LAEF(%) | 29.84±7.91 | 48.74±9.99 | <0.001 |
| LA PLS(%) | 10.70±3.25 | 23.21±6.52 | <0.001 |
注:LAD为左心房前后径;LAVImax为左心房最大容积指数;LAVImin为左心房最小容积指数;LAEF为左心房射血分数;LA PLS为左心房峰值纵向应变 |
表4 血栓组与非血栓组左心耳功能参数比较( |
| 参数 | 血栓组(n=47) | 非血栓组(n=54) | P值 |
|---|---|---|---|
| LAAEV(cm/s) | 29.38±8.10 | 62.99±21.96 | <0.001 |
| LAAD(mm) | 19.21±2.80 | 18.22±2.38 | 0.055 |
| LAAL(mm) | 26.55±5.78 | 26.14±4.95 | 0.702 |
| LAAVmax(ml) | 3.86±1.32 | 3.18±1.23 | 0.009 |
| LAAVmin(ml) | 2.42±0.95 | 1.40±0.63 | <0.001 |
| LAAEF(%) | 38.52±10.71 | 56.10±9.12 | <0.001 |
| LAA PLS(%) | 12.31±3.61 | 25.64±8.81 | <0.001 |
注:LAAEV为左心耳排空速度;LAAD为左心耳口直径;LAAL为左心耳深度;LAAVmax为左心耳最大容积;LAAVmin为左心耳最小容积;LAAEF为左心耳射血分数;LAA PLS为左心耳峰值纵向应变 |
表5 预测血栓形成危险因素的多因素Logistics回归分析 |
| 因素 | β | OR | 95%CI | P值 |
|---|---|---|---|---|
| 持续性心房颤动 | -6.27 | 0.534 | 0.077~3.709 | 0.526 |
| NT-proBNP | 0.003 | 1.003 | 1.000~1.007 | 0.045 |
| LAD | 0.112 | 1.118 | 0.850~1.471 | 0.425 |
| LAVImax | -0.454 | 0.635 | 0.213~1.891 | 0.414 |
| LAVImin | 0.749 | 2.115 | 0.357~12.523 | 0.409 |
| LAEF | 0.146 | 1.157 | 0.691~1.938 | 0.579 |
| LA PLS | -0.373 | 0.668 | 0.515~0.920 | 0.012 |
| LVEF | 0.113 | 1.120 | 0.740~1.695 | 0.592 |
注:NT-proBNP为N-末端脑钠肽前体;LAD为左心房前后径;LAVImax为左心房最大容积指数;LAVImin为左心房最小容积指数;LAEF为左心房射血分数;LA PLS为左心房峰值纵向应变;LVEF为左心室射血分数 |
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
蒋陈晓, 潘忙忙, 杨婷, 等. 非瓣膜性房颤患者左心耳封堵术后抗栓治疗一例[J]. 临床药物治疗杂志, 2021, 19(6): 84-86.
|
| 7 |
庞中一, 谢海秀, 章晔, 等. 心房颤动患者左心房及左心耳血栓形成的危险因素分析[J].心肺血管病杂志, 2017, 36(3): 185-189.
|
| 8 |
黄从新, 张澍, 黄德嘉, 等. 左心耳干预预防心房颤动患者血栓栓塞事件:目前的认识和建议-2019[J].中国心脏起搏与心电生理杂志, 2019, 33(5): 385-401.
|
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
陈银凤, 刘楠楠, 王祖禄, 等. 超声评价左心耳血栓形成的影响因素[J].中国超声医学杂志, 2020, 36(9): 799-801.
|
| 14 |
|
| 15 |
|
| 16 |
徐丽芳, 甘水连, 欧爱玲, 等. 二维斑点追踪成像对非瓣膜性心房颤动患者左房功能的应用价值[J]. 广西医科大学学报, 2019, 36(5): 823-826.
|
| 17 |
|
| 18 |
王菊. 房颤患者左心耳功能及血流动力学改变与其左心耳血栓形成间关系的研究[D]. 河北: 河北医科大学, 2016.
|
| 19 |
李鸿渐, 董小英, 张靖琦, 等. B型脑钠肽对非瓣膜病性心房颤动患者左心耳血栓形成的影响[J].心血管病学进展, 2017, 38(2): 155-158.
|
| 20 |
罗晓颖, 许燕, 张凤如, 等. P波离散度和N端脑钠肽前体预测房颤冷冻球囊导管消融术后复发的价值[J].诊断学理论与实践, 2020, 19(1): 32-36.
|
| 21 |
蔡金, 梁中书, 蒋卫红, 等. 经食管超声心动图评价左心耳血栓与BNP的关系[J].中国超声医学杂志, 2018, 34(2): 143-145.
|
| 22 |
|
| 23 |
张鹏, 张瑞妮, 李飞, 等. B型脑钠肽对老年非瓣膜性房颤病人发生左心耳血栓风险的预测价值[J].中西医结合心脑血管病杂志, 2019, 17(17): 2639-2642.
|
/
| 〈 |
|
〉 |



{kind=link}
{kind=link}
{kind=link}
{kind=link}