
2023 , Vol. 20 >Issue 03: 337 - 342
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.03.014
标准切面质量控制在Ⅲ级产科超声检查胎儿结构异常检出中的应用价值
通信作者:
张波,Email:zora19702006@163.comCopy editor: 吴春凤
收稿日期: 2021-05-24
网络出版日期: 2023-07-05
版权
Application of standard section quality control in improving the detection rate of fetal structural abnormality in second-trimester obstetric ultrasound examination
Corresponding author:
Zhang Bo, Email: zora19702006@163.comReceived date: 2021-05-24
Online published: 2023-07-05
Copyright
探讨超声标准切面质量控制在胎儿结构异常检出中的应用价值。
回顾性分析2018年10月至2020年9月在中日友好医院进行Ⅲ级产科超声检查的4742例孕妇的资料,以开展标准切面质量控制的时间为分界点(2019年10月),将纳入病例分为质量控制前组(B-QC组)和质量控制后组(A-QC组),质量控制内容包括胎儿头颅、胸部、腹部、四肢及附属物的36个标准切面。计算每名孕妇图片存留数目,如图片清晰、切面完整正确则定义为标准切面符合。采用χ2检验比较2组标准切面符合率、胎儿结构异常检出率及漏误诊率有无差别。
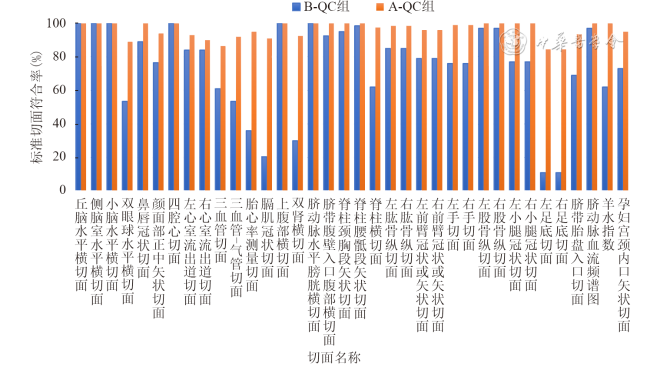
B-QC组平均每名孕妇留存超声图像47张,标准切面符合率平均为73%;A-QC组平均每名孕妇留存超声图像89张,标准切面符合率平均为89%。其中4个标准切面(左足底切面、右足底切面、膈肌冠状切面、双肾横切面)A-QC组较B-QC组检出率明显提高(84.5% vs 11.0%、84.5% vs 11.0%、91.0% vs 20.5%、92.5% vs 30.0%),差异均具有统计学意义(χ2=124.831、124.831、201.475、164.582;P均<0.001)。A-QC组胎儿双眼球水平横切面、鼻唇冠状切面、颜面部正中矢状切面符合率较B-QC组明显提高(89.0% vs 53.5%,100% vs 89.0%,94.0% vs 76.5%),差异均具有统计学意义(χ2=61.523、23.280、24.355;P均<0.001)。A-QC组左心室流出道切面、三血管切面、三血管-气管切面及胎心率测量切面的符合率较B-QC组明显提高(93.0% vs 84.0%,86.5% vs 61.0%,92.0% vs 53.5%,95.0% vs 36.0%),差异均具有统计学意义(χ2=7.959、33.588、74.769、154.044;P均<0.001)。A-QC组超声阳性检出率、胎儿结构异常检出率较B-QC组明显提高(15.7% vs 13.3%,1.3% vs 0.5%),差异具有统计学意义(χ2=7.566、7.571,P均=0.006),漏、误诊率较B-QC组降低(0.8% vs 0.9%,0.2% vs 0.3%),但2组间差异无统计学意义(χ2=1.156、0.269,P=0.604、0.282)。
超声标准切面质量控制通过标准化图片留存和评估,促进了Ⅲ级产科超声检查规范化,提高了超声阳性检出率和胎儿结构异常检出率,为临床决策提供了必要依据。
刘会 , 郑宇觐 , 郭丹丹 , 张波 . 标准切面质量控制在Ⅲ级产科超声检查胎儿结构异常检出中的应用价值[J]. 中华医学超声杂志(电子版), 2023 , 20(03) : 337 -342 . DOI: 10.3877/cma.j.issn.1672-6448.2023.03.014
To evaluate the value of standard section quality control in improving the detection rate of fetal structural abnormality.
A total of 4742 pregnant women who underwent second-trimester obstetric ultrasound examination at our hospital from October 2018 to September 2020 were retrospectively analyzed. Taking the time of beginning to implement quality control as the cutoff point (October 2019), the included cases were divided into either a before-quality control (B-QC) group or an after-quality control (A-QC) group. A total of 36 standard sections of fetal skull, chest, abdomen, limbs, and appendages were analyzed. The number of images retained for each pregnant woman was calculated. If the images were clear and the sections were complete and accurate, the standard sections were defined as image coincidence. The χ2 test was used to compare the coincidence rate of standard sections, the detection rate of fetal structural abnormality, and the rates of missing diagnosis and misdiagnosis between the two groups.
In the B-QC group, there were 47 ultrasonographic images per pregnant woman on average, and the coincidence rate of standard sections was 73%. In the A-QC group, there were 89 ultrasonographic images per pregnant woman on average, and the coincidence rate of standard sections was 89%. The detection rate of four standard sections (left plantar section, right plantar section, diaphragm coronal section, and double kidney transverse section) in the A-QC group was significantly higher than that in the B-QC group (84.5% vs 11.0%, 84.5% vs 11.0%, 91.0% vs 20.5%, and 92.5% vs 30.0%, χ2=124.831, 124.831, 201.475, and 164.582, respectively, P<0.001 for all). Compared with the B-QC group, the coincidence rates of the horizontal transverse section of the eyes, the coronal section of the nose and lip, and the median sagittal section of the face in the A-QC group were significantly higher than those in the B-QC group (89.0% vs 53.5%, 100% vs 89.0%, and 94.0% vs 76.5%, χ2=61.523, 23.280, and 24.355, respectively, P<0.001 for all). The coincidence rates of left ventricular outflow tract section, three-vessel section, three-vessel trachea section, and fetal heart rate section in the A-QC group were significantly higher than those in the B-QC group (93.0% vs 84.0%, 86.5% vs 61.0%, 92.0% vs 53.5%, and 95.0% vs 36.0%, χ2=7.959, 33.588, 74.769, and 154.044, respectively, P<0.001 for all). The detection rates of fetal structural abnormality and fetal malformation in the A-QC group were significantly higher than those in the B-QC group (15.7% vs 13.3% and 1.3% vs 0.5%, χ2=7.566 and 7.571, P=0.006 and 0.006, respectively). The rates of missed and misdiagnosis were decreased (0.8% vs 0.9% and 0.2% vs 0.3%, respectively), but there was no statistical difference between the two groups (χ2=1.156 and 0.269, P=0.604 and 0.282, respectively).
The quality control of the standard sections of ultrasound can improve the coincidence rate of the standardized image retention in grade Ⅲ obstetric ultrasound examination and increase the detection rate of fetal structural abnormality, thus providing a basis for clinical decision-making.
Key words: Ultrasound; Prenatal; Fetal; Malformation; Quality control
表1 Ⅲ级产科超声检查标准切面及观察内容 |
| 分类 | 观察切面 | 解剖结构观察内容 |
|---|---|---|
| 胎头 | 丘脑水平横切面、侧脑室水平横切面、小脑水平横切面 | 颅骨、大脑、大脑镰、透明隔腔、丘脑、第三脑室、侧脑室、小脑半球、小脑蚓部、颅后窝池 |
| 胎儿颜面部 | 双眼球水平横切面、鼻唇冠状切面、颜面部正中矢状切面 | 双眼眶、双眼球、鼻、唇 |
| 胎儿胸部及心脏 | 四腔心切面、左心室流出道切面、右心室流出道切面、三血管切面、三血管-气管切面、胎心率测量切面(多普勒或M型超声) | 胎儿双肺、心胸比值、胎儿心轴、心尖指向、心房、心室、房间隔、室间隔、房室瓣、主动脉、肺动脉 |
| 胎儿膈肌 | 膈肌冠状切面(或左、右膈肌矢状切面) | 膈肌的连续性、腹腔器官及心脏与膈肌的位置关系 |
| 胎儿腹部 | 上腹部横切面、双肾横切面(或左、右肾矢状切面)、脐动脉水平膀胱横切面、脐带腹壁入口处横切面 | 肝、胃、双肾、膀胱、肠道、脐带腹壁入口 |
| 胎儿脊柱 | 脊柱颈胸段矢状切面、脊柱腰骶段矢状切面、脊柱横切面 | 颈段、胸段、腰段、骶尾段脊柱及脊柱生理曲度 |
| 胎儿四肢 | 左、右肱骨纵切面,左、右前臂冠状或矢状切面,左、右手切面;左、右股骨纵切面,左、右小腿冠状切面,左、右足底切面 | 双侧上臂及其内肱骨,双侧前臂及其内尺骨、桡骨,双侧大腿及其内股骨,双侧小腿及其内胫骨、腓骨,双手及双足有无 |
| 胎盘及脐带 | 脐带胎盘入口切面、脐动脉血流频谱图 | 胎盘位置、成熟度、胎盘下缘与宫颈内口的关系、测量胎盘厚度、脐带胎盘及腹壁入口、脐带数目、评估脐动脉血流频谱 |
| 羊水量 | 羊水指数 | 超声探头垂直于水平面,测量区域不能有脐带和肢体 |
| 母体子宫及双附件 | 孕妇宫颈内口矢状切面 | 子宫壁、宫颈管、宫颈内口、双侧附件 |
表2 标准切面质量控制前后Ⅲ级产科超声检查胎儿异常检出情况比较[例(%)] |
| 组别 | 例数 | 胎儿异常 | 软指标阳性 | 结构异常 | 脐血流异常 |
|---|---|---|---|---|---|
| B-QC组 | 2579 | 343(13.3) | 316(12.3) | 14(0.5) | 0(0) |
| A-QC组 | 2163 | 341(15.7) | 305(14.1) | 29(1.3) | 1(0.0) |
| χ2值 | 7.566 | 3.530 | 7.571 | 0.008 | |
| P值 | 0.006 | 0.060 | 0.006 | 0.930 |
注:B-QC为质量控制前组,A-QC为质量控制后组 |
表3 标准切面质量控制前后Ⅲ级产科超声检查中胎儿结构异常分布(例) |
| 结构异常 | 例数 | 结构异常 | 例数 |
|---|---|---|---|
| 质量控制前组 | 肺囊腺瘤 | 3 | |
| 唇裂或唇腭裂 | 3 | 右侧迷走锁骨下动脉 | 2 |
| 21-三体 | 3 | 永存左上腔静脉 | 2 |
| 颅后窝囊肿 | 1 | 房室间隔缺损缺 | 1 |
| 隔离肺 | 1 | 室间隔缺损 | 1 |
| 多囊肾 | 1 | 右位主动脉弓 | 1 |
| 肾积水 | 1 | 肠梗阻 | 1 |
| 持续性右脐静脉 | 1 | 腹部囊性包块 | 1 |
| 软骨发育不全 | 1 | 肾积水 | 1 |
| 多发畸形 | 1 | 重复肾 | 1 |
| 双胎畸形 | 1 | 开放性脊柱裂 | 1 |
| 质量控制后组 | 足内翻 | 1 | |
| 唇裂或唇腭裂 | 5 | 软骨发育不全 | 1 |
| 持续性右脐静脉 | 5 | 多发畸形 | 1 |
| 1 |
姚莉琴, 邹团标, 张山山, 等. 1986~2014年中国出生缺陷发生率的变化趋势及地理分布 [J]. 中国优生与遗传杂志, 2020, 28(3): 351-356
|
| 2 |
|
| 3 |
朱霞, 陈欣林, 杨小红, 等. 开展胎儿系统超声筛查的研究意义 [J]. 中国产前诊断杂志(电子版), 2013, 5(4): 3-6
|
| 4 |
中国医师协会超声医师分会. 产前超声检查指南(2012) [J/CD]. 中华医学超声杂志(电子版), 2012, 9(7): 574-580.
|
| 5 |
荆春丽, 丁伟, 孙寒冰, 等. 超声在中孕期筛查胎儿唇裂及唇腭裂的价值 [J/CD]. 中华医学超声杂志(电子版), 2013, 10(4): 286-291.
|
| 6 |
李胜利, 罗国阳. 胎儿畸形产前超声诊断学 [M]. 2版. 北京: 科学出版社, 2017: 91-136.
|
| 7 |
|
| 8 |
李胜利, 文华轩. 中孕期胎儿系统超声检查切面及临床意义 [J/CD]. 中华医学超声杂志(电子版), 2010, 7(3): 366-381.
|
| 9 |
|
| 10 |
李国政, 庄松岩, 李智瑶, 等. 胎儿肢体及手足畸形产前超声诊断及图像分析 [J/CD]. 中华医学超声杂志(电子版), 2014, 11(1): 53-60.
|
/
| 〈 |
|
〉 |

{kind=link}
{kind=link}