
2023 , Vol. 20 >Issue 04: 404 - 410
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.04.005
二维斑点追踪成像评价左束支起搏左心室激动顺序与同步性
Copy editor: 汪荣
收稿日期: 2021-08-24
网络出版日期: 2023-08-07
基金资助
四川省卫生健康委科技项目(20PJ210)
版权
Evaluation of left ventricular activation sequence and intraventricular synchronization in patients with left bundle branch pacing by two-dimensional speckle tracking imaging
Received date: 2021-08-24
Online published: 2023-08-07
Copyright
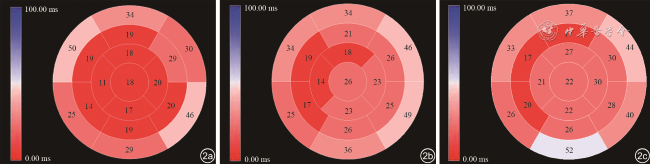
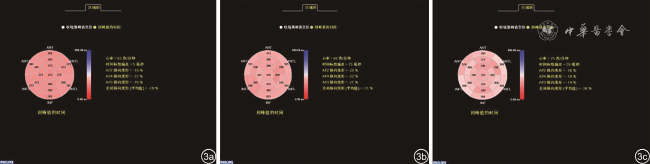
应用二维斑点追踪成像(2D-STI)对左束支起搏(LBBP)左心室激动顺序进行间接标测,并分析室内同步性。
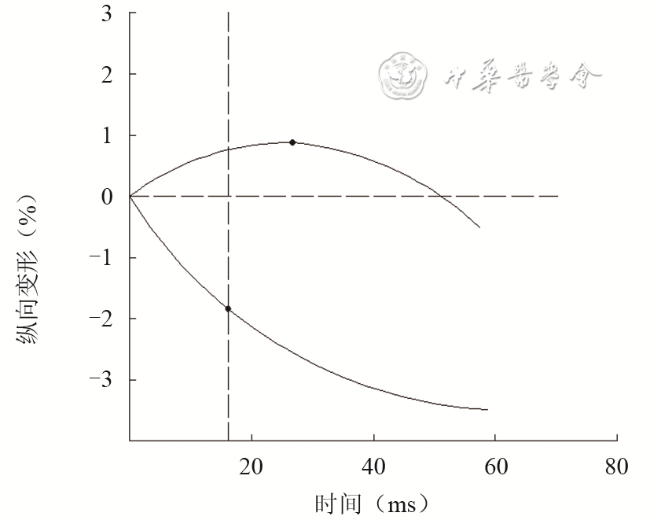
选取2020年7月至2020年12月于成都市第三人民医院成功进行LBBP的患者22例(LBBP组)和右心室流出道起搏(RVOTP)患者16例(RVOTP组),2组患者均于术后3个月随诊复查超声心动图。另选取健康成年人17例作为对照组。采用2D-STI生成应变-时间曲线,收缩早期正向曲线收缩起始时间(OTS)为心电图R波峰至正向应变达峰时间;记录负向曲线第二帧时的应变绝对值(Sn),以Sn中取值最大者(S)和第二帧时间(T)计算收缩早期应变速度(V=S/T),OTS=T-Sn/V。采用整体及各水平纵向应变达峰时间标准差(Tp-SD)作为室内同步性参数。
正常组QRS时限最短(95.35±10.04)ms,LBBP组次之(113.41±11.46)ms,RVOTP组明显延长(144.94±13.03)ms,差异均有统计学意义(P均<0.05)。各水平OTS相比较,仅RVOTP组侧壁心尖段与正常组差异有统计学意义[(29.56±13.33)ms vs(19.53±15.02)ms,P<0.05]。各组最早激动节段的OTS值以正常组最小(10.76±9.67)ms,LBBP组次之(14.45±7.30)ms,RVOTP组最大(17.19±19.43)ms。各组最早与最晚激动节段OTS之差均在40 ms以内。RVOTP组整体、中间段Tp-SD与LBBP组、正常组相比差异均有统计学意义(P均<0.05),而基底段、心尖段Tp-SD比较差异均无统计学意义(P均>0.05);LBBP组各水平Tp-SD与正常组比较差异均无统计学意义(P均>0.05)。
2D-STI可无创地标测左心室激动顺序,有助于发现激动顺序的异常改变;LBBP术后早期可维持相对正常的左心室激动顺序和室内同步性,且同步性明显优于RVOTP。
王秀秀 , 严霜霜 , 邓晓奇 , 熊峰 . 二维斑点追踪成像评价左束支起搏左心室激动顺序与同步性[J]. 中华医学超声杂志(电子版), 2023 , 20(04) : 404 -410 . DOI: 10.3877/cma.j.issn.1672-6448.2023.04.005
To map the left ventricular activation sequence indirectly and analyze the intraventricular synchronization in patients with left bundle branch pacing (LBBP) by two-dimensional speckle tracking imaging (2D-STI).
Twenty-two patients with LBBP and 16 patients with right ventricular outflow tract pacing (RVOTP) in Chengdu Third People's Hospital from July 2020 to December 2020 were enrolled, and 17 healthy adults were selected as a control group. Strain-time curves were generated by 2D-STI. Onset time of systole (OTS) of positive curves was the time from the R wave to the positive peak strain. For negative curves, the largest value (S) of absolute strain values (Sn) at the second frame and the second frame time (T) were used to calculate the strain rate (V=S/T), and OTS was calculated as T-Sn/V. The standard deviation of peak time (Tp-SD) was used as the intraventricular synchronization parameter.
QRS duration was the shortest in the control group [(95.35±10.04) ms], followed by the LBBP group [(113.41±11.46) ms], and it was significantly prolonged in the RVOTP group [(144.94±13.03) ms]; the difference between any two groups was statistically significant (P<0.05). When comparing OTS at all levels, only OTS in the apical segment of lateral wall in the RVOTP group was significantly different from that in the control group [(29.56±13.33) ms vs (19.53±15.02) ms, P<0.05]. OTS of the earliest excited segment was the lowest in the control group [(10.76±9.67) ms], followed by the LBBP group [(14.45±7.30) ms] and RVOTP group [(17.19±19.43) ms]. The difference of OTS between the earliest and the latest excited segments in each group was less than 40 ms. Compared with the LBBP group and the control group, Tp-SD in the global and middle segment was statistically different in the RVOTP group (P<0.05), but there was no significant difference in Tp-SD in the basal segment and apical segment (P>0.05). There was no significant difference in Tp-SD between the LBBP group and the control group (P<0.05).
2D-STI can noninvasively map the left ventricular activation sequence and assist to find the change of activation sequence. LBBP can maintain relatively normal left ventricular activation sequence and intraventricular synchronization in the early stage after operation, and the synchronization is significantly better than that by RVOTP.
表1 LBBP组、RVOTP组与正常组一般资料比较 |
| 一般资料 | 正常组(n=17) | LBBP组(n=22) | RVOTP组(n=16) | 统计值 | P值 |
|---|---|---|---|---|---|
| 年龄(岁, ±s) | 59.65±9.53 | 66.32±12.78 | 68.19±12.13 | F=2.514 | 0.091 |
| 性别[男性,例(%)] | 10(58.8) | 13(59.1) | 10(62.5) | χ2=0.059 | 0.971 |
| 心率(次/分, ±s) | 73.82±8.22 | 70.32±9.02 | 69.47±8.20 | H=4.720 | 0.094 |
| 起搏指征 | χ2=1.000 | 0.604 | |||
| Ⅱ度Ⅱ型AVB[例,(%)] | - | 8(36.4) | 6(37.5) | ||
| Ⅲ度AVB[例,(%)] | - | 14(63.6) | 10(62.5) | ||
| 基础疾病 | |||||
| 高血压[例,(%)] | - | 12(54.5) | 6(37.5) | χ2=2.663 | 0.264 |
| 糖尿病[例,(%)] | - | 8(36.4) | 5(31.3) | χ2=0.233 | 0.890 |
| QRS时限(ms, ±s) | 95.35±10.04 | 113.41±11.46a | 144.94±13.03ab | F=77.080 | <0.001 |
注:LBBP为左束支起搏;RVOTP为右心室流出道起搏;AVB为房室传导阻滞;与正常组比较,aP<0.05;与LBBP组比较,bP<0.05;-表示无数据 |
表2 LBBP组、RVOTP组与正常组常规超声心动图参数比较( |
| 超声心动图参数 | 正常组(n=17) | LBBP组(n=22) | RVOTP组(n=16) | 统计值 | P值 |
|---|---|---|---|---|---|
| IVSd(mm) | 9.59±0.94 | 10.14±1.13 | 9.88±0.96 | F=2.239 | 0.326 |
| LVPWd(mm) | 9.69±0.87 | 10.19±0.91 | 10.00±1.21 | F=1.261 | 0.292 |
| LVDd(mm) | 43.06±2.38 | 45.45±3.22 | 45.06±4.28 | F=2.668 | 0.079 |
| LVSd(mm) | 29.63±2.60 | 31.31±3.55 | 30.25±3.09 | F=2.224 | 0.118 |
| LAD(mm) | 35.00±3.13 | 36.64±3.53 | 35.81±2.99 | H=4.134 | 0.127 |
| LVEF(%) | 63.59±2.21 | 61.45±1.71 | 62.81±5.46 | H=5.832 | 0.054 |
注:LBBP为左束支起搏;RVOTP为右心室流出道起搏;IVSd为室间隔厚度;LVPWd为左心室后壁厚度;LVDd为左心室舒张末期内径;LVSd为左心室收缩末期内径;LAD为左心房内径;LVEF为左心室射血分数 |
表3 LBBP组、RVOTP组与正常组基底段OTS比较(ms, |
| 组别 | 例数 | 前壁 | 侧壁 | 后壁 | 下壁 | 后间壁 | 前间壁 |
|---|---|---|---|---|---|---|---|
| 正常组 | 17 | 33.60±31.48 | 29.65±27.50 | 45.94±30.81 | 29.24±34.05 | 24.94±27.47 | 50.35±29.65 |
| LBBP组 | 22 | 34.09±28.75 | 45.73±32.32 | 49.48±36.33 | 35.68±28.54 | 25.27±26.10 | 33.50±25.29 |
| RVOTP组 | 16 | 36.69±18.60 | 43.94±22.37 | 40.25±35.24 | 52.13±43.70 | 26.33±34.66 | 33.38±31.02 |
| H值 | 1.043 | 2.970 | 0.835 | 4.005 | 0.669 | 3.644 | |
| P值 | 0.549 | 0.227 | 0.659 | 0.135 | 0.716 | 0.162 |
注:OTS为收缩起始时间;LBBP为左束支起搏;RVOTP为右心室流出道起搏 |
表4 LBBP组、RVOTP组与正常组中间段OTS比较(ms, |
| 组别 | 例数 | 前壁 | 侧壁 | 后壁 | 下壁 | 后间壁 | 前间壁 |
|---|---|---|---|---|---|---|---|
| 正常组 | 17 | 19.18±23.24 | 29.06±34.89 | 20.41±21.08 | 19.18±21.19 | 13.71±15.50 | 19.24±14.45 |
| LBBP组 | 22 | 21.41±22.35 | 25.76±21.94 | 24.59±15.01 | 26.45±25.09 | 16.64±13.21 | 19.09±14.58 |
| RVOTP组 | 16 | 17.19±19.43 | 29.50±29.31 | 27.81±20.04 | 26.31±28.21 | 19.88±25.30 | 17.25±13.95 |
| H值 | 0.428 | 0.249 | 3.276 | 0.607 | 1.995 | 0.847 | |
| P值 | 0.807 | 0.883 | 0.194 | 0.738 | 0.369 | 0.665 |
注:OTS为收缩起始时间;LBBP为左束支起搏;RVOTP为右心室流出道起搏 |
表5 LBBP组、RVOTP组与正常组心尖段OTS比较(ms, |
| 组别 | 例数 | 前壁 | 侧壁 | 下壁 | 室间隔 | 心尖帽 |
|---|---|---|---|---|---|---|
| 正常组 | 17 | 18.47±11.03 | 19.53±15.02 | 16.65±15.54 | 10.76±9.67 | 17.82±11.31 |
| LBBP组 | 22 | 18.32±5.69 | 22.77±9.89 | 22.86±11.40 | 14.45±7.30 | 25.77±10.12 |
| RVOTP组 | 16 | 27.00±30.27 | 29.56±13.33a | 21.63±22.02 | 21.00±22.73 | 22.06±13.04 |
| 统计值 | H=0.942 | H=7.943 | H=4.052 | H=3.157 | F=2.337 | |
| P值 | 0.624 | 0.019 | 0.132 | 0.206 | 0.107 |
注:OTS为收缩起始时间;LBBP为左束支起搏;RVOTP为右心室流出道起搏;与正常组比较,aP<0.05 |
表6 LBBP组、RVOTP组与正常组各水平Tp-SD比较(ms, |
| 组别 | 例数 | 整体 | 基底段 | 中间段 | 心尖段 |
|---|---|---|---|---|---|
| 正常组 | 17 | 38.02±4.67 | 40.56±3.89 | 36.40±3.49 | 36.90±6.16 |
| LBBP组 | 22 | 40.39±3.18 | 41.65±4.17 | 40.22±2.52 | 39.09±2.47 |
| RVOTP组 | 16 | 46.80±7.08ab | 44.91±2.42 | 51.80±9.57 ab | 43.08±4.33 |
| 统计值 | H=21.097 | F=2.403 | H=13.053 | H=5.360 | |
| P值 | <0.001 | 0.124 | 0.001 | 0.069 |
注:Tp-SD为纵向应变达峰时间标准差;LBBP为左束支起搏;RVOTP为右心室流出道起搏;与正常组比较,aP<0.05;与LBBP组比较,bP<0.05 |
特别感谢黄山市人民医院心电功能检查科胡敏副主任医师对本研究的专业技术指导。
| 1 |
|
| 2 |
|
| 3 |
中华医学会心电生理和起搏分会, 中国医师协会心律学专业委员会. 希氏-浦肯野系统起搏中国专家共识 [J]. 中华心律失常学杂志, 2021, 25(1): 10-36.
|
| 4 |
胡敏, 江成璠, 王素霞, 等. 使用心肌机械运动顺序间接标测左室电激动顺序的临床研究 [J]. 中国心脏起搏与心电生理杂志, 2016, 30(3): 229-233.
|
| 5 |
|
| 6 |
|
| 7 |
|
| 8 |
严霜霜, 邓晓奇, 熊峰, 等. 二维斑点追踪技术评价左束支区域起搏早期左心室收缩功能及同步性 [J/CD]. 中华医学超声杂志(电子版), 2021, 18(4): 368-374.
|
| 9 |
张丽娟, 邓晓奇, 王淑珍, 等. 实时三维超声心动图对比评价左束支区域起搏与右室流出道起搏术后左室整体收缩功能及同步性 [J]. 临床超声医学杂志, 2021, 23(5): 347-350.
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
徐亮. 右室不同部位起搏的左室激动顺序及收缩同步性对心功能影响的实验研究 [D]. 南京: 南京医科大学, 2011: 1-52.
|
| 16 |
|
/
| 〈 |
|
〉 |



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}