
2023 , Vol. 20 >Issue 08: 787 - 794
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.08.001
超声衰减参数成像评价儿童代谢相关脂肪性肝病的价值
Copy editor: 汪荣
收稿日期: 2022-03-28
网络出版日期: 2023-10-31
基金资助
广东省高水平医院建设专项经费资助(深儿医科教科【2023】7号)
深圳市科技创新委员会基础研究(自由探索)项目(JCYJ20180228175150018)
版权
Evaluation of metabolic dysfunction-associated fatty liver disease in children by ultrasound-guided attenuation parameter
Received date: 2022-03-28
Online published: 2023-10-31
Copyright
探讨超声衰减参数成像(UGAP)评价儿童代谢相关脂肪性肝病(MAFLD)病变程度的价值。
回顾性选取2022年5月至2023年2月在深圳市儿童医院就诊的肥胖症患儿131例,包括MAFLD组76例、单纯肥胖组55例,同期选取性别、年龄匹配的健康体检儿童58例为正常对照组。比较各组间及不同程度脂肪肝患儿衰减系数(AC)的差异,应用相关比率Eta2和Spearman相关分析法探讨AC值与脂肪肝程度、体质量指数(BMI)、纤维化指数(FIB-4指数)及实验室指标的相关性,通过多因素Logistic回归分析构建MAFLD预测模型并进行诊断效能分析。
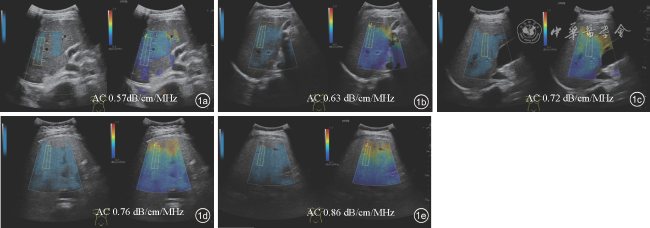
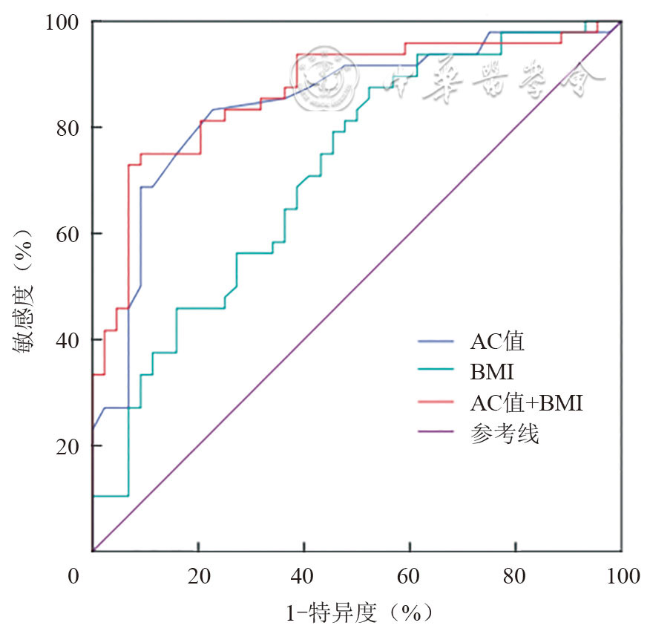
MAFLD组、单纯肥胖组和正常对照组AC值分别为(0.758±0.076)、(0.637±0.039)、0.575(0.560,0.590)dB/cm/MHz,组间差异有统计学意义(P均<0.05)。轻度、中度及重度脂肪肝患儿的AC值分别为(0.728±0.067)、(0.789±0.070)、(0.858±0.041)dB/cm/MHz,组间差异有统计学意义(P均<0.05)。AC值与脂肪肝程度呈强相关(Eta2=0.586),与BMI呈中等相关(rs=0.422,P<0.001),与FIB-4指数无相关性(rs=-0.080、P=0.58),AC值联合BMI的模型预测MAFLD的ROC曲线下面积为0.869。模型最佳预测截点值为AC≥0.675 dB/cm/MHz、BMI≥22.05 kg/m2。
肝脏AC值在单纯肥胖及MAFLD儿童中均有增高,反映了肝脏脂肪变性的程度;UGAP定量AC值联合BMI可作为肥胖儿童预测MAFLD的危险因素。UGAP可作为临床筛查、诊断、评估肝脂肪变性严重程度及监测其进展的有效工具。
刘婷婷 , 林妍冰 , 汪珊 , 陈幕荣 , 唐子鉴 , 代东伶 , 夏焙 . 超声衰减参数成像评价儿童代谢相关脂肪性肝病的价值[J]. 中华医学超声杂志(电子版), 2023 , 20(08) : 787 -794 . DOI: 10.3877/cma.j.issn.1672-6448.2023.08.001
To evaluate the value of ultrasound-guided attenuation parameter (UGAP) for evaluating the degree of metabolic dysfunction-associated fatty liver disease (MAFLD) in children.
One hundred and thirty-one children in which obesity was confirmed at Shenzhen Children's Hospital between May 2022 and February 2023 were retrospectively selected. According to the ultrasound findings, the patients were divided into two groups: MAFLD group (n=76) and simple obesity group (n=55). Fifty-eight sex- and age-matched healthy children were selected as a control group. The attenuation coefficient (AC) was compared among all groups and different hepatic steatosis grades. Correlation ratio (Eta2) and Spearman's correlation coefficient were used to assess the correlation between AC and the grade of hepatic steatosis, body mass index (BMI), fibrosis-4 (FIB-4) index, and laboratory indices. Multivariate logistic regression analysis was used to construct an MAFLD predictive model. The diagnostic performance of the predictive model was evaluated by receiver operating characteristic (ROC) curve analysis.
AC values in the MAFLD, simple obesity, and normal control groups were (0.758±0.076), (0.637±0.039), and 0.575 (0.560, 0.590) dB/cm/MHz, respectively. AC values in the patients with mild, moderate, and severe fatty liver were (0.728±0.067), (0.789±0.070), and (0.858±0.041) dB/cm/MHz, respectively. There were significant differences in AC values among different groups and hepatic steatosis grades ( P<0.05 for all). There was a highly significant correlation between AC values and hepatic steatosis grades (Eta2=0.586); a moderate correlation between AC values and BMI (rs=0.422, P<0.001); but no correlation between AC values and FIB-4 index (rs=-0.080, P=0.58). The equation of the MAFLD predictive model was: Logistic (P) = -22.081+0.242X (100AC)+0.233X (BMI). The area under the curve of the predictive model was 0.869. The cut-off values were AC ≥ 0.675 dB/cm/MHz and BMI ≥ 22.05 kg/m2.
AC values in the liver increase in children with simple obesity and those with MAFLD, which could reflect the grade of hepatic steatosis. AC values quantified using UGAP and BMI are predictors of MAFLD in children with obesity. UGAP might be an effective tool for clinical screening, diagnosis, and evaluation of hepatic steatosis severity and monitoring its progression.
 表示,组间进行独立样本t检验或单因素方差分析;非正态分布的计量资料用M(Q1,Q3)表示,组间进行Mann-Whitney U检验或Kruskal-Wallis H检验。计数资料采用χ2检验。采用相关比率Eta2分析AC值与脂肪肝程度的相关程度,当Eta2<0.06时,表明变量之间的相关程度微弱;0.06≤Eta2≤0.16,表明变量之间有中度的相关关系;Eta2>0.16时,表明变量之间存在强相关;采用Spearman相关分析AC值与BMI、FIB-4指数、实验室指标的相关性,相关系数r<0.2表明变量之间几乎无相关;0.2≤r<0.4表明变量之间轻度相关;0.4≤r<0.7表明变量之间中等程度相关;r≥0.7表明变量之间强相关。将单因素分析中差异有统计学意义的变量纳入多因素Logistic回归分析,建立MAFLD预测模型,采用ROC曲线评价模型价值。采用组内相关系数(intra-class correlation coefficient,ICC)进行AC值观察者内及观察者间变异度检验。以P<0.05为差异有统计学意义。
表示,组间进行独立样本t检验或单因素方差分析;非正态分布的计量资料用M(Q1,Q3)表示,组间进行Mann-Whitney U检验或Kruskal-Wallis H检验。计数资料采用χ2检验。采用相关比率Eta2分析AC值与脂肪肝程度的相关程度,当Eta2<0.06时,表明变量之间的相关程度微弱;0.06≤Eta2≤0.16,表明变量之间有中度的相关关系;Eta2>0.16时,表明变量之间存在强相关;采用Spearman相关分析AC值与BMI、FIB-4指数、实验室指标的相关性,相关系数r<0.2表明变量之间几乎无相关;0.2≤r<0.4表明变量之间轻度相关;0.4≤r<0.7表明变量之间中等程度相关;r≥0.7表明变量之间强相关。将单因素分析中差异有统计学意义的变量纳入多因素Logistic回归分析,建立MAFLD预测模型,采用ROC曲线评价模型价值。采用组内相关系数(intra-class correlation coefficient,ICC)进行AC值观察者内及观察者间变异度检验。以P<0.05为差异有统计学意义。表1 MAFLD组、单纯肥胖组及正常对照组一般资料比较 |
| 组别 | 例数 | 男性[例(%)] | 年龄[岁,M(Q1,Q3), ] ] | BMI[kg/m2,M(Q1,Q3), ] ] | FIB-4( ) ) |
|---|---|---|---|---|---|
| MAFLD组 | 76 | 55(21) | 10.80(9.70,12.40) | 25.58±5.07 | 0.18±0.06 |
| 单纯肥胖组 | 55 | 39(16) | 10.37±1.92 | 22.54±4.36a | 0.18±0.07 |
| 正常对照组 | 58 | 35(23) | 10.46±2.13 | 18.05(15.20,22.76)ab | - |
| 统计值 | χ2=2.330 | H=4.341 | H=40.271 | t=0.441 | |
| P值 | 0.312 | 0.114 | <0.001 | 0.661 |
注:MAFLD为代谢相关脂肪性肝病;BMI为体质量指数;FIB-4为肝纤维化指数;与MAFLD组比较,aP<0.05;与单纯肥胖组比较,bP<0.05;-为无相关数据 |
表2 MAFLD组与单纯肥胖组实验室指标比较 |
| 组别 | 例数 | TC(mmol/L, ) ) | LDL-C[mmol/L, ,M(Q1,Q3)] ,M(Q1,Q3)] | TG(mmol/L, ) ) | |
|---|---|---|---|---|---|
| MAFLD组 | 76 | 4.32±0.86 | 2.89±0.84 | 1.40±0.67 | |
| 单纯肥胖组 | 55 | 4.12±0.60 | 2.49(2.23,3.02) | 1.07±0.45 | |
| 统计值 | t=-1.285 | Z=774.500 | t=-2.768 | ||
| P值 | 0.202 | 0.067 | 0.007 | ||
| 组别 | 例数 | HDL-C(mmol/L, ) ) | FBG[mmol/L, ,M(Q1,Q3)] ,M(Q1,Q3)] | ALT[IU/L,M(Q1,Q3)] | AST[IU/L,M(Q1,Q3)] |
| MAFLD组 | 76 | 1.13±0.18 | 4.60(4.43,4.90) | 33.0(24.5,62.0) | 27.0(21.0,37.0) |
| 单纯肥胖组 | 55 | 1.24±0.21 | 4.83±0.34 | 17.0(14.0,27.0) | 22.0(18.0,24.0) |
| 统计值 | t=2.631 | Z=471.500 | Z=472.500 | Z=712.000 | |
| P值 | 0.010 | 0.076 | <0.001 | 0.001 | |
注:MAFLD为代谢相关脂肪性肝病;TC为总胆固醇;LDL-C为低密度脂蛋白胆固醇;TG为甘油三酯;HDL-C为高密度脂蛋白胆固醇;FBG为空腹血糖;ALT为丙氨酸转氨酶;AST为天冬氨酸转氨酶 |
表3 AC值联合BMI预测MAFLD的Logistic回归分析 |
| 相关因素 | β值 | SE值 | Wald χ2值 | P值 | OR值(95%CI) |
|---|---|---|---|---|---|
| 100AC值 | 0.242 | 0.063 | 14.647 | <0.001 | 1.274(1.125~1.442) |
| BMI | 0.233 | 0.097 | 5.806 | 0.016 | 1.263(1.044~1.526) |
| 常数 | -22.081 | 5.358 | 16.983 | <0.001 |
注:AC为衰减系数;BMI为体质量指数;MAFLD为代谢相关脂肪性肝病;β为回归系数;SE为标准误;Wald为瓦尔德值;OR为优势比;CI为置信区间 |
| 1 |
张薇,魏来. 非酒精性脂肪性肝病在亚洲的流行情况 [J]. 中华肝脏病杂志, 2013, 21(11): 801-804.
|
| 2 |
濮佳琦, 王森杰, 薛初晴, 等. 儿童脂肪性肝病命名探析 [J]. 中华儿科杂志, 2023, 61(2): 104-107.
|
| 3 |
|
| 4 |
|
| 5 |
中华医学会儿科学分会内分泌遗传代谢学组,中华医学会儿科学分会消化学组,中华医学会儿科学分会青春期医学专业委员会,等. 儿童非酒精性脂肪肝病诊断与治疗专家共识 [J]. 中国实用儿科杂志, 2018, 33(7): 487-492.
|
| 6 |
中华医学会肝病学分会脂肪肝和酒精性肝病学组,中国医师协会脂肪性肝病专家委员会.非酒精性脂肪性肝病防治指南(2018年更新版) [J]. 临床肝胆病杂志, 2018, 34(5): 947-957.
|
| 7 |
|
| 8 |
中华医学会儿科学分会内分泌遗传代谢学组,中华医学会儿科学分会儿童保健学组, 中华医学会儿科学分会临床营养学组,等. 中国儿童肥胖诊断评估与管理专家共识 [J]. 中华儿科杂志, 2022, 60(6): 507-515.
|
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
|
| 17 |
|
| 18 |
|
| 19 |
包静文,朱宇莉,徐庆玥,等. 超声声衰减成像评估代谢相关脂肪性肝病肝脂肪变程度的应用价值 [J]. 中华超声影像学杂志, 2021, 30(10): 868-873.
|
| 20 |
|
| 21 |
张姝嫔,程成,祝怡婕,等. 超声衰减成像定量诊断非酒精性脂肪肝的应用价值初探讨 [J]. 中国超声医学杂志, 2021, 37(1): 66-69.
|
| 22 |
|
| 23 |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}