
2023 , Vol. 20 >Issue 10: 1016 - 1022
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.10.003
心肌收缩早期延长对非ST段抬高型急性冠脉综合征患者冠状动脉严重狭窄的预测价值
Copy editor: 汪荣
收稿日期: 2022-09-26
网络出版日期: 2024-01-08
版权
Value of myocardial early systolic lengthening in non-ST-segment elevation acute coronary syndrome for predicting severe coronary artery stenosis
Received date: 2022-09-26
Online published: 2024-01-08
Copyright
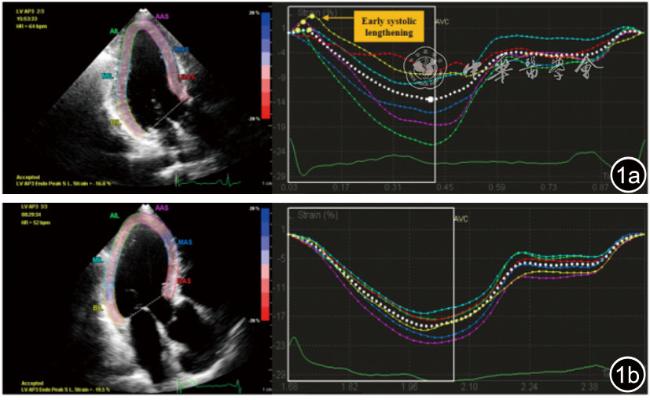
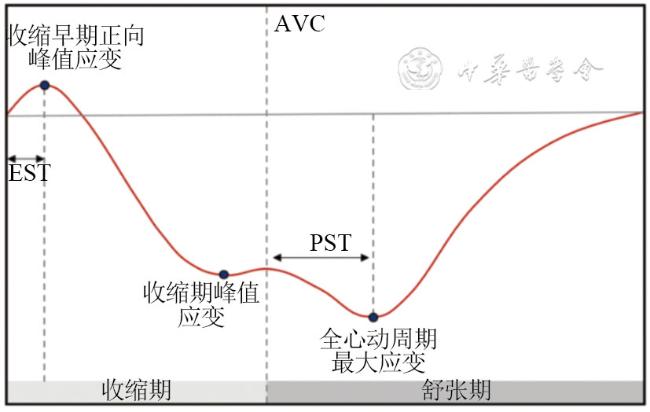
应用二维斑点追踪成像(2D-STl)评价无节段性室壁运动异常的非ST段抬高型急性冠脉综合征(NSTE-ACS)患者的左心室心肌整体及区域收缩早期延长(ESL),探讨ESL参数对冠状动脉严重狭窄的预测价值。
纳入2019年2月至2019年6月首都医科大学附属北京朝阳医院收治的冠脉造影前行超声心动图检查的无节段性室壁运动异常的NSTE-ACS患者171例。根据冠脉造影结果将其分为冠状动脉严重狭窄组123例(至少一支冠状动脉直径狭窄≥70%)和冠状动脉非严重狭窄组48例(各分支冠状动脉直径狭窄<70%)。应用2D-STI获得左心室心肌整体纵向应变(GLS)、整体收缩早期延长时间(GEST)、整体收缩后时间(GPST)及左心室心肌区域纵向应变(TLS),区域收缩早期延长时间(TEST)和区域收缩后时间(TPST),比较两组间的上述参数。应用ROC曲线分析整体和区域参数对冠状动脉严重狭窄的诊断效能,确定曲线下面积(AUC)和截断值。通过Logistic回归分析NSTE-ACS患者冠状动脉严重狭窄的独立影响因素。
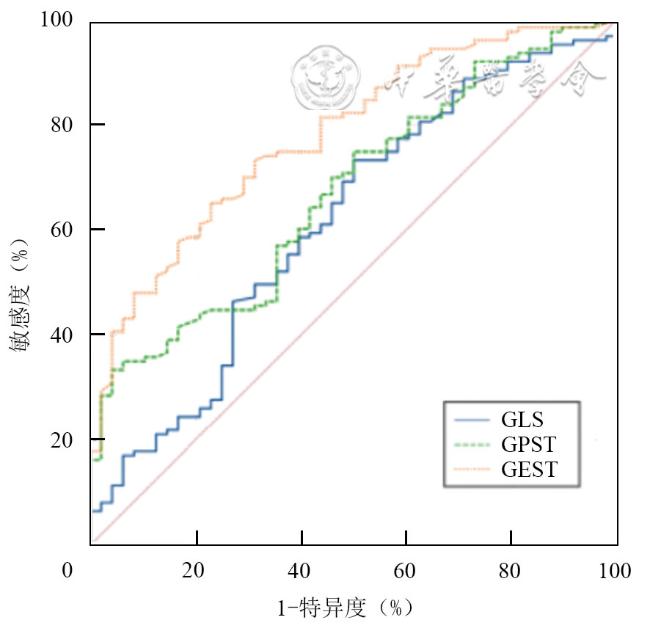
与非严重狭窄组相比,冠状动脉严重狭窄患者的GEST、GPST增大,GLS减低(P均<0.05)。严重狭窄冠状动脉灌注区的TEST、TPST较非严重狭窄冠状动脉灌注区增大(P均<0.001),而TLS差异无统计学意义(P=0.227)。心肌GEST>8.9 ms预测冠状动脉严重狭窄的AUC为0.78(敏感度65%,特异度77%),大于GLS(AUC=0.62)和GPST(AUC=0.67);TEST对严重狭窄冠状动脉灌注区也具有一定区分能力(AUC=0.62,敏感度72%,特异度51%)。心肌GEST是冠状动脉严重狭窄的独立预测因素。
NSTE-ACS冠状动脉严重狭窄患者的左心室整体及区域收缩功能受损,心肌GEST、TESL增大。ESL参数是早期识别无明显室壁运动异常的NSTE-ACS患者存在冠状动脉严重狭窄的可靠依据。
张婉微 , 秦芸芸 , 蔡绮哲 , 林明明 , 田润雨 , 金姗 , 吕秀章 . 心肌收缩早期延长对非ST段抬高型急性冠脉综合征患者冠状动脉严重狭窄的预测价值[J]. 中华医学超声杂志(电子版), 2023 , 20(10) : 1016 -1022 . DOI: 10.3877/cma.j.issn.1672-6448.2023.10.003
To analyze the early systolic lengthening (ESL) of the left ventricular myocardium by two-dimensional speckle tracking imaging (2D-STI) in non-ST-segment elevation acute coronary syndrome (NSTE-ACS) patients who had no regional wall motion abnormality, and to explore the predictive value of global and territorial ESL for severe coronary artery stenosis.
A total of 171 NSTE-ACS patients without obvious regional wall motion abnormality who underwent echocardiography before coronary angiography at Beijing Chaoyang Hospital Affiliated to Capital Medical University from February to June 2019 were enrolled. According to the degree of coronary stenosis, there were 123 subjects in severe coronary artery stenosis group (≥70% diameter stenosis in at least one coronary artery) and 48 subjects in non-severe coronary stenosis group (<70% diameter narrowing in every coronary artery branch). Left ventricular myocardial global longitudinal strain (GLS), time to global early systolic lengthening (GEST), time to global post-systolic shorting (GPST) and territorial longitudinal strain (TLS), time to territorial early systolic lengthening (TEST), and time to territorial post-systolic shorting (TPST) were obtained by 2D-STI. The differences in the above parameters were compared between the two groups. Receiver operating characteristic (ROC) curve analysis was performed to assess the diagnostic efficacy of global and regional parameters for severe coronary artery stenosis by determining their area under the ROC curve (AUC) and cut-off values. A logistic regression model was established to determine the independent predictors of severe coronary stenosis in NSTE-ACS patients.
Compared with the non-severe coronary artery stenosis group, left ventricular GEST and GPST were significantly increased, while GLS was significantly decreased in NSTE-ACS patients with severe coronary artery stenosis (P<0.05 for all). In addition, both myocardial TEST and TPST were significantly increased in regions supplied by severely stenotic coronary arteries compared to non-severely stenotic coronary arteries (P<0.001 for both), while there was no statistically significant difference in left ventricular TLS between regions supplied by severely stenotic coronary arteries and non-severely stenotic coronary arteries (P=0.227). ROC curve analysis showed that myocardial GEST>8.9 ms yielded a specificity of 65% and sensitivity of 77%, and had the highest AUC (0.78) in predicting severe coronary stenosis, superior to GLS (AUC=0.62, P<0.05) and GPST (AUC=0.67, P<0.05). In addition, myocardial TEST could also distinguish regions related to severe coronary artery stenosis and non-severe arteries with moderate diagnostic accuracy (AUC=0.62, sensitivity 72%, specificity 51%). In multivariable logistic regression analysis, only left ventricular myocardial GEST remained an independent predictor of severe coronary artery stenosis in patients with NSTE-ACS.
In NSTE-ACS patients with severe coronary artery stenosis, left ventricular global and territorial systolic function are impaired, and particularly, both myocardial GEST and TEST are significantly increased. ESL parameters may be a reliable index for predicting severe coronary stenosis in NSTE-ACS patients without obvious regional wall motion abnormality.
 或M(QR)表示,组间比较采用独立样本t检验或秩和检验,计数资料以例(%)表示,采用χ2检验比较组间差异。应用ROC曲线分析整体和区域参数对冠状动脉严重狭窄的诊断效能,确定曲线下面积(area under the curve,AUC)和截断值。通过Logistic回归分析NSTE-ACS患者冠状动脉严重狭窄的独立影响因素。观察者内及观察者间的一致性分析采用组内相关系数(intraclass correlation coefficients,ICC)。以P<0.05为差异有统计学意义。
或M(QR)表示,组间比较采用独立样本t检验或秩和检验,计数资料以例(%)表示,采用χ2检验比较组间差异。应用ROC曲线分析整体和区域参数对冠状动脉严重狭窄的诊断效能,确定曲线下面积(area under the curve,AUC)和截断值。通过Logistic回归分析NSTE-ACS患者冠状动脉严重狭窄的独立影响因素。观察者内及观察者间的一致性分析采用组内相关系数(intraclass correlation coefficients,ICC)。以P<0.05为差异有统计学意义。表1 冠状动脉严重狭窄组与非严重狭窄组一般资料及常规超声心动图参数比较 |
| 组别 | 例数 | 年龄(岁, ) ) | 男性[例(%)] | 高血压[例(%)] | 糖尿病[例(%)] | 高血脂[例(%)] | LVEDV(ml, ) ) | LVESV(ml, ) ) | LVEF(%, ) ) | E/e'( ) ) |
|---|---|---|---|---|---|---|---|---|---|---|
| 非严重狭窄组 | 48 | 63.2±8.7 | 27(56.3) | 31(64.6) | 13(27.1) | 43(89.6) | 73.5±15.6 | 27.5±6.4 | 62.1±2.9 | 11.4±3.8 |
| 严重狭窄组 | 123 | 63.6±8.8 | 75(61.0) | 92(74.8) | 56(45.5) | 108(87.8) | 73.6±18.1 | 28.8±8.4 | 61.4±3.6 | 11.7±3.8 |
| 统计值 | t=0.288 | χ2=0.320 | χ2=1.784 | χ2=4.880 | χ2=0.106 | t=0.041 | t=-0.978 | t=1.302 | t=-0.488 | |
| P值 | 0.773 | 0.571 | 0.182 | 0.027 | 0.745 | 0.967 | 0.330 | 0.195 | 0.626 |
注:LVEDV为左心室舒张末期容积;LVESV为左心室收缩末期容积;LVEF为左心室射血分数;E/e'为舒张早期二尖瓣峰值流速与二尖瓣环平均运动速度的比值 |
表2 冠状动脉严重狭窄组与非严重狭窄组左心室整体心肌形变参数比较 |
| 组别 | 例数 | GLS(%, ) ) | GEST[ms,M(QR)] | GPST[ms,M(QR)] |
|---|---|---|---|---|
| 非严重狭窄组 | 48 | -18.5±2.1 | 5.6(7.0) | 15.4(18.5) |
| 严重狭窄组 | 123 | -17.6±2.4 | 11.5(8.4) | 22.3(29.3) |
| 统计值 | t=-2.339 | Z=-5.650 | Z=-3.491 | |
| P值 | 0.020 | <0.001 | 0.003 |
注:GLS为整体纵向应变;GEST为整体收缩早期延长时间;GPST为整体收缩后时间 |
表3 严重狭窄冠状动脉灌注区与非严重狭窄灌注区心肌形变参数比较 |
| 组别 | 个数 | TLS(%, ) ) | TEST[ms,M(QR)] | TPST[ms,M(QR)] |
|---|---|---|---|---|
| 非严重狭窄灌注区 | 311 | -17.7±3.0 | 6.6(12.9) | 16.8(21.8) |
| 严重狭窄灌注区 | 202 | -17.4±3.2 | 10.6(12.1) | 23.9(34.2) |
| 统计值 | t=-1.210 | Z=-4.737 | Z=-3.491 | |
| P值 | 0.227 | <0.001 | <0.001 |
注:TLS为区域纵向应变;TEST为区域收缩早期延长时间;TPST为区域收缩后时间 |
表4 整体和区域心肌形变参数预测冠状动脉严重狭窄的效能分析 |
| 参数 | AUC(95%CI) | 截断值 | 敏感度(%) | 特异度(%) | 约登指数 | P值 |
|---|---|---|---|---|---|---|
| GLS | 0.62(0.50~0.71) | -18.9% | 73 | 50 | 0.23 | <0.05 |
| GPST | 0.67(0.60~0.74) | 36.0 ms | 33 | 95 | 0.28 | <0.05 |
| GEST | 0.78(0.71~0.84) | 8.9 ms | 65 | 77 | 0.42 | <0.05 |
| TLS | 0.53(0.48~0.57) | -15.3% | 25 | 82 | 0.07 | >0.05 |
| TPST | 0.61(0.57~0.65) | 30.7 ms | 39 | 78 | 0.17 | <0.05 |
| TEST | 0.62(0.58~0.67) | 6.8 ms | 72 | 51 | 0.23 | <0.05 |
注:GLS为整体纵向应变;GEST为整体收缩早期延长时间;GPST为整体收缩后时间;TLS为区域纵向应变;TEST为区域收缩早期延长时间;TPST为区域收缩后时间 |
表5 预测NSTE-ACS患者冠状动脉严重狭窄的单因素及多因素Logistic回归分析 |
| 变量 | 单因素Logistic回归 | 多因素Logistic回归 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 回归系数 | 标准误 | Wald卡方值 | OR值 | P值 | 回归系数 | 标准误 | Wald卡方值 | OR值 | P值 | |
| 糖尿病 | 0.81 | 0.37 | 4.76 | 2.25 | 0.029 | 0.38 | 0.42 | 0.80 | 1.46 | 0.371 |
| GLS | 0.18 | 0.08 | 5.18 | 1.20 | 0.023 | 0.18 | 0.10 | 3.72 | 1.20 | 0.054 |
| GPST | 0.04 | 0.01 | 12.08 | 1.05 | 0.001 | 0.02 | 0.01 | 2.74 | 1.02 | 0.098 |
| GEST | 0.20 | 0.04 | 24.98 | 1.23 | <0.001 | 0.18 | 0.04 | 16.70 | 1.20 | <0.001 |
注:GLS为整体纵向应变;GEST为整体收缩早期延长时间;GPST为整体收缩后时间 |
| 1 |
中华医学会心血管病学分会, 中华心血管病杂志编辑委员会. 非ST段抬高型急性冠状动脉综合征诊断和治疗指南(2016) [J]. 中华心血管病杂志, 45(5): 359-376.
|
| 2 |
|
| 3 |
|
| 4 |
陈银花, 陈勇, 马勇, 等. 分层应变技术评价非 ST 段抬高性急性冠状动脉综合征患者左心室心肌各层收缩功能的变化 [J/CD]. 中华医学超声杂志(电子版), 2017, 14(12): 919-926.
|
| 5 |
张清凤, 王胰, 张红梅, 等. 二维斑点追踪参数在平板运动负荷超声中的应用研究 [J/CD]. 中华超声医学杂志(电子版), 2020, 17(8): 753-758.
|
| 6 |
|
| 7 |
|
| 8 |
|
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
|
| 17 |
|
| 18 |
|
| 19 |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}