
2023 , Vol. 20 >Issue 11: 1107 - 1113
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.11.001
高帧频超声造影在膀胱癌分级及分期中的应用价值
Copy editor: 吴春凤
收稿日期: 2023-09-26
网络出版日期: 2024-01-15
版权
Clinical application of high-frame-rate contrast-enhanced ultrasound in grading and staging of bladder cancer
Received date: 2023-09-26
Online published: 2024-01-15
Copyright
探讨高帧频超声造影(H-CEUS)在评估膀胱癌不同分级与分期的应用价值。
回顾性分析2023年1月至3月解放军总医院第一医学中心的23例膀胱癌患者的H-CEUS特征,并与病理检查结果对照。按照病理级别分为低级别尿路上皮癌(LGUC)组与高级别尿路上皮癌(HGUC)组;按照病理分期分为非肌层浸润性膀胱癌(NMIBC)组和肌层浸润性膀胱癌(MIBC)组。采用t检验分析不同分级2组间及不同分期2组间患者的年龄、病灶不同径线大小的差异;采用Fisher精确检验分析不同分级2组间及不同分期2组间在H-CEUS下观察到的血管支数、血管形态、微泡直接进入病灶的膀胱壁来源层面及病灶基底处膀胱壁固有肌层完整性的差异。
LGUC组(12例)与HGUC组(11例)比较,LGUC组的血管支数多为1~2支(66.7%,8/12),而HGUC组多为≥3支(54.5%,6/11),差异具有统计学意义(P=0.010);LGUC组膀胱壁固有肌层完整的占83.3%(10/12),而HGUC组膀胱壁固有肌层多不完整(72.7%,8/11),差异具有统计学意义(P=0.012)。LGUC组与HGUC组患者年龄、病灶不同径线大小、血管形态、微泡直接进入病灶的膀胱壁来源层面比较,差异均无统计学意义(P均>0.05)。NMIBC组(16例)与MIBC组(7例)比较,NMIBC组病灶内的血管支数多为1~2支(68.7%,11/16),而MIBC组多为≥3支(57.1%,4/7),差异具有统计学意义(P=0.003);NMIBC组与MIBC组相比,微泡多从黏膜层直接进入病灶(75.0% vs 14.3%,P=0.019);MIBC组与NMIBC组相比,固有肌层全部不完整(100% vs 18.7%,P<0.001)。NMIBC组与MIBC组病灶不同径线大小、基底部宽度及血管形态比较,差异均无统计学意义(P均>0.05)。
H-CEUS大大提高了造影帧频,能较大程度上呈现肿瘤的灌注细节,为膀胱癌分级及分期带来新的诊断价值。
池梦婷 , 赵萍 , 李静波 , 朱嘉宁 , 宋禄达 , 罗渝昆 , 李秋洋 . 高帧频超声造影在膀胱癌分级及分期中的应用价值[J]. 中华医学超声杂志(电子版), 2023 , 20(11) : 1107 -1113 . DOI: 10.3877/cma.j.issn.1672-6448.2023.11.001
To evaluate the clinical value of high-frame-rate contrast-enhanced ultrasound (H-CEUS) in grading and staging bladder cancer.
The H-CEUS features of 23 patients with bladder cancer treated at the First Medical Center, Chinese PLA General Hospital from January to March 2023 were retrospectively analyzed and compared with pathological examination results. According to pathological grades, the patients were divided into a low grade urothelium carcinoma (LGUC) group and a high grade urothelium carcinoma (HGUC) group. According to pathological stages, the patients were divided into a non-muscular invasive bladder cancer (NMIBC) group and a muscular invasive bladder cancer (MIBC) group. The t test was used to compare the difference in age and tumor diameter between patients with different grades and different stages. The Fisher exact test was used to analyze the differences in the number of vascular branches, vascular morphology, the source bladder wall layer from which microbubbles directly entering the lesion, and the integrity of the intrinsic muscle layer of the bladder wall at the base of the lesion observed by H-CEUS between patients with different grades and different stages.
The number of visible blood vessels within the lesion in the LGUC group (n=12) was mostly 1-2 (66.7%, 8/12), while it was ≥ 3 (54.5%, 6/11) in the HGUC group (n=11), with a statistically significant difference between the two groups (P=0.01). The percentage of patients with an intact mucosal layer was 83.3% (10/12) in the LGUC group, while it was 27.3% (3/11) in the HGUC group, with a statistically significant difference between the two groups (P=0.012). There was no significant difference between the LGUC group and HGUC group in patient’s age, lesion size, vascular morphology, and the source bladder wall layer from which microbubbles directly entering the lesion (P>0.05). The number of vessels in the NMIBC group (n=16) was 1-2 (68.7%, 11/16), while it was ≥ 3 (57.1%, 4/7) in the MIBC group (n=7), with a statistically significant difference between the two groups (P=0.003). Compared to MIBC, NMIBC had more microbubbles that entered into the lesion directly from the mucosal layer (75.0% vs 14.3%, P=0.019). Compared to NMIBC, MIBC mostly had an incomplete intrinsic muscle layer (100% vs 18.7%, P<0.001). There was no statistically significant difference between the NMIBC group and MIBC group in terms of lesion diameter, basal width, and vascular morphology.
H-CEUS greatly improves the contrast frame frequency, presents the perfusion details of the tumor to a large extent, and brings new diagnostic value to the staging and grading of bladder cancer.
Key words: High-frame-rate; Contrast-enhanced ultrasound; Bladder cancer
 表示,组间比较采用t检验,不符合正态分布的计量资料以M(QR)表示,组间比较采用Mann Whitney U非参数检验;计数资料以频率表示,采用Fisher精确检验进行组间比较。P<0.05为差异具有统计学意义。
表示,组间比较采用t检验,不符合正态分布的计量资料以M(QR)表示,组间比较采用Mann Whitney U非参数检验;计数资料以频率表示,采用Fisher精确检验进行组间比较。P<0.05为差异具有统计学意义。表1 NMIBC组与MIBC组以及LGUC组与HGUC组患者一般临床资料比较 |
| 组别 | 例 | 男性/女性(例) | 年龄(岁, ) ) | 血尿(有/无,例) |
|---|---|---|---|---|
| NMIBC组 | 16 | 16/0 | 64.88±11.55 | 13/3 |
| MIBC组 | 7 | 5/2 | 64.71±7.52 | 6/1 |
| 统计值 | - | t=0.034 | - | |
| P值 | 0.083 | 0.491 | 1.000 | |
| LGUC组 | 12 | 12/0 | 65.33±12.91 | 10/2 |
| HGUC组 | 11 | 9/2 | 64.27±7.09 | 10/1 |
| 统计值 | - | t=0.241 | - | |
| P值 | 0.217 | 0.321 | 1.000 |
注:LGUC为低级别尿路上皮癌,HGUC为高级别尿路上皮癌,NMIBC为非肌层浸润性膀胱癌,MIBC为肌层浸润性膀胱癌;-表示无相应统计值,采用Fisher检验 |
表2 NMIBC组与MIBC组常规超声图像及H-CEUS特征比较 |
| 特征 | NMIBC(16例) | MIBC(7例) | 统计值 | P值 |
|---|---|---|---|---|
| 病理级别(例) | - | 0.027 | ||
| LGUC | 11 | 1 | ||
| HGUC | 5 | 6 | ||
| 平行径[cm,M(QR)] | 2.30(1.95,2.98) | 2.70(2.20,4.50) | Z=1.341 | 0.198 |
| 垂直径[cm,M(QR)] | 1.50(1.20,1.83) | 1.80(1.00,2.00) | Z=0.201 | 0.871 |
| 基底宽[cm,M(QR)] | 1.45(0.43,0.70) | 2.20(1.60,3.60) | Z=2.283 | 0.022 |
| 垂直径/平行径[M(QR)] | 0.70(0.55,0.83) | 0.74(0.38,1.86) | Z=0.000 | 1.000 |
| H-CEUS显示血管数(例) | - | 0.003 | ||
| 0支 | 5 | 0 | ||
| 1~2支 | 11 | 3 | ||
| ≥3支 | 0 | 4 | ||
| H-CEUS显示血管形态(例) | - | 0.124 | ||
| 点状 | 6 | 0 | ||
| 不规则 | 10 | 7 | ||
| H-CEUS显示微泡路径(例) | - | 0.019 | ||
| 仅来源于黏膜层 | 12 | 1 | ||
| 非仅来源于黏膜层 | 4 | 6 | ||
| 固有肌层完整性(例) | - | <0.001 | ||
| 完整 | 13 | 0 | ||
| 不完整 | 3 | 7 |
注:NMIBC为非肌层浸润性膀胱癌;MIBC为肌层浸润性膀胱癌;H-CEUS为高帧频超声造影;-表示无相应统计值,采用Fisher检验 |
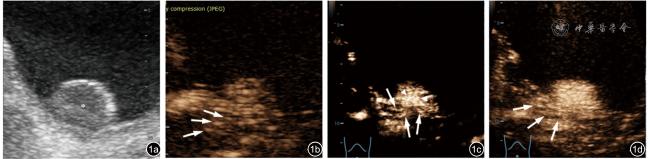
图1 1例54岁男性肌层浸润性膀胱癌患者常规超声及高帧频超声造影图像。图a:常规超声可见膀胱壁上一低回声病灶(*);图b:非黏膜层来源微泡进入病灶内部(↑);图c:病灶基底部多支血管影(↑),病灶内亦可见不规则血管影(▲);图d:病灶基底部固有肌层显示不完整(↑) |
表3 LGUC组与HGUC组常规超声图像及H-CEUS特征比较 |
| 特征 | LGUC(12例) | HGUC(11例) | 统计值 | P值 |
|---|---|---|---|---|
| 平行径[cm,M(QR)] | 2.30(1.95,3.48) | 2.50(2.20,2.70) | Z =0.556 | 0.608 |
| 垂直径[cm,M(QR)] | 1.55(1.23,2.58) | 1.40(1.00,1.80) | Z =-1.573 | 0.118 |
| 基底宽[cm,M(QR)] | 1.45(0.35,1.68) | 2.00(0.70,2.20) | Z =1.794 | 0.079 |
| 垂直径/平行径[M(QR)] | 0.75(0.66,0.86) | 0.64(0.32,0.74) | Z =-2.001 | 0.044 |
| H-CEUS显示血管数(例) | - | 0.010 | ||
| 0支 | 4 | 1 | ||
| 1~2支 | 8 | 4 | ||
| ≥3支 | 0 | 6 | ||
| H-CEUS显示血管形态(例) | - | 0.155 | ||
| 点状 | 5 | 1 | ||
| 不规则 | 7 | 10 | ||
| H-CEUS显示微泡路径(例) | - | 1.000 | ||
| 仅来源于黏膜层 | 9 | 4 | ||
| 非仅来源于黏膜层 | 3 | 7 | ||
| 固有肌层完整性(例) | - | 0.012 | ||
| 完整 | 10 | 3 | ||
| 不完整 | 2 | 8 |
注:LGUC为低级别尿路上皮癌;HGUC为高级别尿路上皮癌;H-CEUS为高帧频超声造影;-表示无相应统计值,采用Fisher检验 |
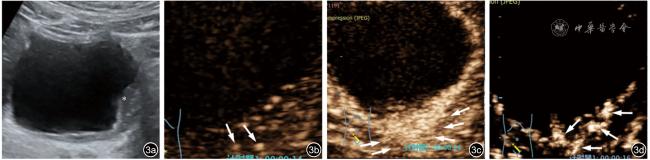
图3 一例67岁男性高级别尿路上皮癌患者常规超声及高帧频超声造影图像。图a:常规超声可见膀胱壁低回声病灶(*);图b:病灶内非黏膜层来源的微泡声像图(↑);图c:动脉期显示不完整的固有肌层(↑);图d:病灶内多支形态不规则血管影(↑) |
| 1 |
|
| 2 |
|
| 3 |
朱嘉宁, 李静波, 罗渝昆, 等. 常规超声及超声造影在肾上腺肿瘤诊断中的应用 [J]. 中国研究型医院, 2022, 9(3): 57-60.
|
| 4 |
魏群, 蔡静宜, 罗晋, 等. 超声引导下真空辅助切除乳腺病灶的多中心队列真实世界研究 [J]. 中国研究型医院, 2023, 10(1): 39-44.
|
| 5 |
费翔, 罗渝昆, 李楠, 等. 高帧频超声造影在肝富血供占位性病变动脉期中的成像优势与临床价值 [J/OL]. 中华医学超声杂志(电子版), 2020, 17(9): 827-833.
|
| 6 |
韩鹏, 费翔, 罗渝昆, 等. 高帧频超声造影在鉴别诊断胆囊腺瘤性息肉与胆固醇性息肉中的临床应用 [J/OL]. 中华医学超声杂志(电子版), 2020, 17(9): 815-820.
|
| 7 |
梁舒媛, 罗渝昆, 费翔, 等. 高帧频超声造影在鉴别浅表淋巴结性质中的应用 [J/OL]. 中华医学超声杂志(电子版), 2020, 17(9): 841-847.
|
| 8 |
李楠, 梁舒媛, 费翔, 等. 高帧频超声造影对颈动脉粥样硬化斑块内新生血管的评价价值 [J/OL]. 中华医学超声杂志(电子版), 2020, 17(9): 854-859.
|
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
李秋洋, 唐杰, 何恩辉, 等. 超声造影在鉴别膀胱上皮癌分级中的应用价值 [J]. 中国医学科学院学报, 2012, 34(4): 364-368.
|
| 15 |
|
| 16 |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}