
2024 , Vol. 21 >Issue 02: 158 - 162
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2024.02.008
超声心动图诊断胎儿单纯肺动脉瓣狭窄的价值
Copy editor: 汪荣
收稿日期: 2023-10-26
网络出版日期: 2024-04-25
版权
Value of echocardiography in diagnosis of isolated fetal pulmonary valvular stenosis
Received date: 2023-10-26
Online published: 2024-04-25
Copyright
探讨超声心动图在诊断胎儿单纯肺动脉瓣狭窄(PVS)中的价值。
回顾性分析2019年1月至2022年12月在天津市中心妇产科医院超声科和承德医学院附属医院南区超声科产前经超声心动图诊断为单纯PVS的胎儿35例。胎儿心脏超声检查获取四腔心切面、左心室及右心室流出道切面、三血管切面等。测量各心腔横径,观察房室瓣启闭及反流情况。出生的胎儿均于产后24 h内行超声心动图检查,测量肺动脉速度和肺动脉跨瓣压差,评估肺动脉瓣狭窄程度。分析产前和产后超声心动图检查结果,采用Pearson相关分析产前PVS分组(正向组、逆向组)与产后PVS分度(轻、中、重度)之间的相关性。
35例单纯PVS胎儿引产8例,出生27例。产前动脉导管(DA)正向组15例,逆向组20例,2组病例肺动脉流速、肺动脉狭窄后扩张和三尖瓣反流程度差异具有统计学意义(P<0.05)。肺动脉内径,左、右肺动脉内径,肺动脉瓣开口和右心室横径/左心室横径差异无统计学意义(P>0.05)。27例出生后新生儿期超声心动图检查均证实有不同程度PVS,轻度15例,中度8例,重度4例。产前PVS不同分组与产后PVS不同分度之间具有相关性(Pearson相关系数=0.58,P<0.05),产前正向组病例产后大部分为轻度PVS(12/14,85.71%),逆向组病例产后中度和重度PVS居多(10/13,76.92%)。
胎儿单纯PVS肺动脉流速快,三尖瓣反流程度重,DA逆灌产后可能中度以上PVS的可能性大,狭窄后扩张是胎儿PVS的一个重要间接征象。胎儿单纯PVS可以在产前进行诊断,超声心动图是诊断胎儿单纯PVS并预估其产后分度的重要手段。
李博 , 彭芳华 , 孔德璇 , 张欢欢 , 曲东辉 , 王锟 , 阚长利 , 聂明辉 , 刘天鑫 , 吴文瑛 . 超声心动图诊断胎儿单纯肺动脉瓣狭窄的价值[J]. 中华医学超声杂志(电子版), 2024 , 21(02) : 158 -162 . DOI: 10.3877/cma.j.issn.1672-6448.2024.02.008
To assess the value of echocardiography in the diagnosis of isolated fetal pulmonary valvular stenosis (PVS).
From January 2019 to December 2022, 35 fetuses diagnosed with PVS by prenatal echocardiography at the Department of Ultrasound of Tianjin Central Obstetrics and Gynecology Hospital and the Department of Ultrasound of Southern District of Chengde Medical College were retrospectively analyzed. Fetal echocardiography was performed to obtain four chamber sections, left ventricular and right ventricular outflow tract sections, and three vessel sections. The transverse diameter of each heart cavity was measured, and the opening and closing of the atrioventricular valve and regurgitation were observed. All fetuses were examined by echocardiography within 24 h after delivery to measure pulmonary artery velocity and pulmonary artery cross-valve pressure difference and evaluate the degree of pulmonary artery stenosis. The results of prenatal and postnatal echocardiography were analyzed, and Pearson correlation was used to analyze the correlation between prenatal PVS grouping (forward group and reverse group) and postpartum PVS grading (mild, moderate, and severe).
Of the 35 fetuses with PVS included, 8 underwent induced labor and 27 were born. There were 15 cases in the forward prenatal ductus arteriae (DA) group and 20 cases in the reverse prenatal DA group, and there were statistically significant differences in pulmonary artery velocity, dilation of the pulmonary artery after stenosis, and tricuspid regurgitation between the two groups (P<0.05). There was no significant difference in pulmonary artery diameter, left and right pulmonary artery diameter, pulmonary valve opening, and right ventricular diameter/left ventricular diameter ratio (P>0.05). All 27 cases of PVS in neonatal period were confirmed by echocardiography, of which 15 were mild, 8 were moderate, and 4 were severe. There was a correlation between different groups of prenatal PVS and different grades of postpartum PVS (Pearson correlation coefficient=0.58, P<0.05). Mild PVS (12/14 85.71%) was found mainly in the positive prenatal group, while moderate and severe PVS (10/13 76.92%) was found predominantly in the reverse group.
Pulmonary artery velocity is fast and tricuspid valve regurgitation is severe in fetuses with isolated PVS. The possibility of moderate or higher PVS is high after DA reverse perfusion. Dilation after stenosis is an important indirect sign of fetal PVS. Fetal PVS alone can be diagnosed before birth, and echocardiography is an important means to diagnose isolated fetal PVS and estimate its postpartum grade.
Key words: Echocardiography; Fetus; Pulmonary valve stenosis; Prenatal; Postpartum
 表示,2组间比较采用独立样本t检验。计数资料以例(%)表示,2组间比较采用χ2检验。产前PVS分组与产后PVS分度之间的相关性分析采用Pearson相关系数检验。以P<0.05为差异有统计学意义。
表示,2组间比较采用独立样本t检验。计数资料以例(%)表示,2组间比较采用χ2检验。产前PVS分组与产后PVS分度之间的相关性分析采用Pearson相关系数检验。以P<0.05为差异有统计学意义。表1 8例引产胎儿超声心动图表现 |
| 病例序号 | 诊断孕龄(周) | 肺动脉瓣情况 | 肺动脉狭窄后扩张 | 肺动脉瓣开口(mm) | 肺动脉流速(cm/s) | 三尖瓣反流 | 动脉导管血流 | 右心增大 | 右心室壁增厚 |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 25+1 | 回声增强、增厚,启闭受限 | 有 | 2.1 | 316 | 大量 | 逆向 | 无 | 无 |
| 2 | 38+5 | 回声增强、增厚,启闭受限 | 有 | 3.0 | 322 | 大量 | 逆向 | 有 | 有 |
| 3 | 29+6 | 回声增强、增厚,启闭受限 | 有 | 2.8 | 351 | 大量 | 逆向 | 有 | 无 |
| 4 | 23+6 | 回声增强、增厚 | 有 | 2.0 | 311 | 中量 | 逆向 | 无 | 无 |
| 5 | 23+4 | 回声增强、增厚 | 有 | 1.1 | 232 | 少量 | 逆向 | 无 | 无 |
| 6 | 26+4 | 回声增强、增厚 | 有 | 2.0 | 253 | 大量 | 逆向 | 有 | 无 |
| 7 | 25+5 | 回声增强、增厚 | 无 | 2.1 | 207 | 少量 | 无 | 无 | 无 |
| 8 | 24+3 | 回声增强、增厚,启闭受限 | 有 | 2.0 | 315 | 中量 | 逆向 | 无 | 无 |
图1 胎儿单纯肺动脉瓣狭窄超声心动图图像。图a示胎儿肺动脉瓣增厚、回声增强,启闭略受限;图b示胎儿肺动脉前向血流略呈花彩;图c示肺动脉流速>140 cm/s;图d示肺动脉狭窄后扩张,动脉导管血流逆向灌注肺动脉 |
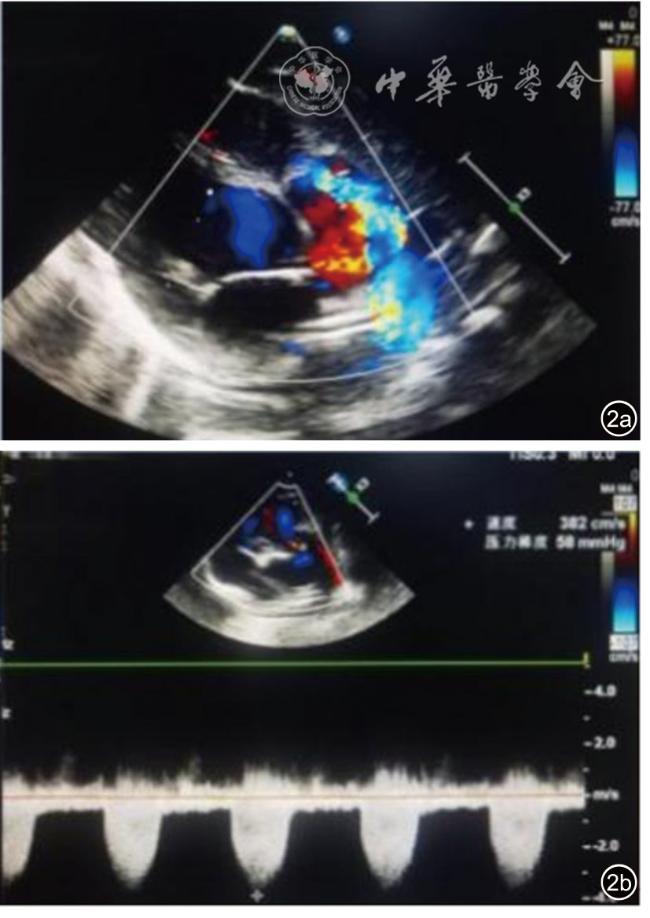
图2 新生儿肺动脉瓣狭窄(中度)超声心动图图像。图a示肺动脉瓣增厚、回声增强,启闭受限;彩色多普勒血流成像(CDFI)示前向血流呈花彩;图b示流速为382 cm/s,跨瓣压差为58 mmHg |
表2 正向组与逆向组单纯PVS胎儿超声心动图结果比较 |
| 超声心动图参数 | 正向组(n=15) | 逆向组(n=20) | 统计值 | P值 |
|---|---|---|---|---|
肺动脉瓣流速(m/s, ) ) | 171.27±23.70 | 273.20±47.59 | t=-7.60 | <0.01 |
肺动脉内径(mm, ) ) | 5.02±1.13 | 4.55±1.21 | t=1.16 | 0.26 |
左肺动脉内径(mm, ) ) | 2.71±0.44 | 3.09±0.73 | t=0.34 | 0.08 |
右肺动脉内径(mm, ) ) | 2.82±0.53 | 3.05±0.69 | t=-1.08 | 0.29 |
肺动脉瓣开口(mm, ) ) | 2.77±0.70 | 3.44±3.92 | t=0.64 | 0.52 |
右心室横径/左心室横径( ) ) | 0.95±0.27 | 1.07±0.18 | t=-1.65 | 0.11 |
| 三尖瓣反流[例(%)] | χ2=11.67 | <0.01 | ||
| 轻度及以下 | 13(86.7) | 8(40.0) | ||
| 中度 | 2(13.3) | 7(35.0) | ||
| 重度 | 0 | 5(25.0) | ||
| 肺动脉狭窄后扩张[例(%)] | 8(53.3) | 20(100.0) | χ2=13.40 | <0.01 |
注:PVS为肺动脉瓣狭窄 |
表3 27例单纯PVS产前不同分组与产后不同分度之间的相关性分析 |
| 胎儿单纯PVS分组 | 例数 | 产后单纯PVS 分度(例) | Pearson相关系数 | P值 | ||
|---|---|---|---|---|---|---|
| 轻度 | 中度 | 重度 | ||||
| 正向组 | 14 | 12 | 2 | 0 | 0.58 | <0.01 |
| 逆向组 | 13 | 3 | 6 | 4 | ||
| 合计 | 27 | 15 | 8 | 4 | ||
注:PVS为肺动脉瓣狭窄 |
| [1] |
|
| [2] |
接连利, 许燕, 程建, 等.胎儿单纯性肺动脉狭窄的声像图特征及其诊断价值[J].中华超声影像学杂志, 2012, 21(21): 1082-1083.
|
| [3] |
王颖玉, 庞程程, 申俊君, 等.胎儿肺动脉瓣狭窄产前诊断、治疗与转归的临床研究[J].岭南心血管病杂志, 2023, 29(2): 144-149.
|
| [4] |
国家卫生健康委员会国家结构性心脏病介入质量控制中心, 国家心血管病中心结构性心脏病介入质量控制中心, 中华医学会心血管病学分会先心病经皮介入治疗指南工作组, 等.常见先天性心脏病经皮介入治疗指南(2021版) [J].中华医学杂志, 2021, 101(38): 3054-3076.
|
| [5] |
广东省预防医学会出生缺陷预防与控制专业委员会, 中华医学会儿科分会心血管病学组胎儿心脏病协作组.胎儿超声心动图检查技术规范(2021版) [J]. 岭南心血管病杂志, 2022, 28(3): 282-286.
|
| [6] |
|
| [7] |
董凤群. 超声五切面筛查胎儿心脏结构异常 [J/CD]. 中华医学超声杂志 (电子版), 2018, 15(12): 881-900.
|
| [8] |
|
/
| 〈 |
|
〉 |

{kind=link}
{kind=link}
{kind=link}
{kind=link}