
2024 , Vol. 21 >Issue 06: 585 - 592
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2024.06.006
二尖瓣空间变化联合左心房应变对肥厚型心肌病合并左心室流出道梗阻的预测价值
Copy editor: 汪荣
收稿日期: 2024-03-19
网络出版日期: 2024-08-05
基金资助
四川省科技厅-四川省自然科学基金(2023NSFSC0641)
四川省人民医院苗圃课题(2015MP34)
版权
Predictive value of mitral valve spatial changes combined with left atrial strain for left ventricular outflow tract obstruction in patients with hypertrophic cardiomyopathy
Received date: 2024-03-19
Online published: 2024-08-05
Copyright
联合二尖瓣空间参数和左心房应变参数,探讨静息超声心动图相关参数对肥厚型心肌病(HCM)合并左心室流出道梗阻(LVOTO)的预测价值。
回顾性纳入2021年1月至2023年12月在四川省人民医院门诊或住院期间行超声心动图确诊为HCM的患者95例。获取临床资料、常规超声心动图参数、二尖瓣空间参数和左心房应变参数。依据静息时和激发后左心室流出道压力阶差(LVOTG)将研究对象分为非梗阻性HCM 49例和梗阻性HCM 46例两组,比较各参数的组间差异。对单因素分析组间差异有统计学意义的二尖瓣及左心房参数进行ROC曲线分析,计算曲线下面积,获得最佳截断值及其敏感度和特异度。将ROC曲线分析有统计学意义的参数纳入多因素Logistic回归分析,获得HCM合并LVOTO的独立预测因素及其预测效能。
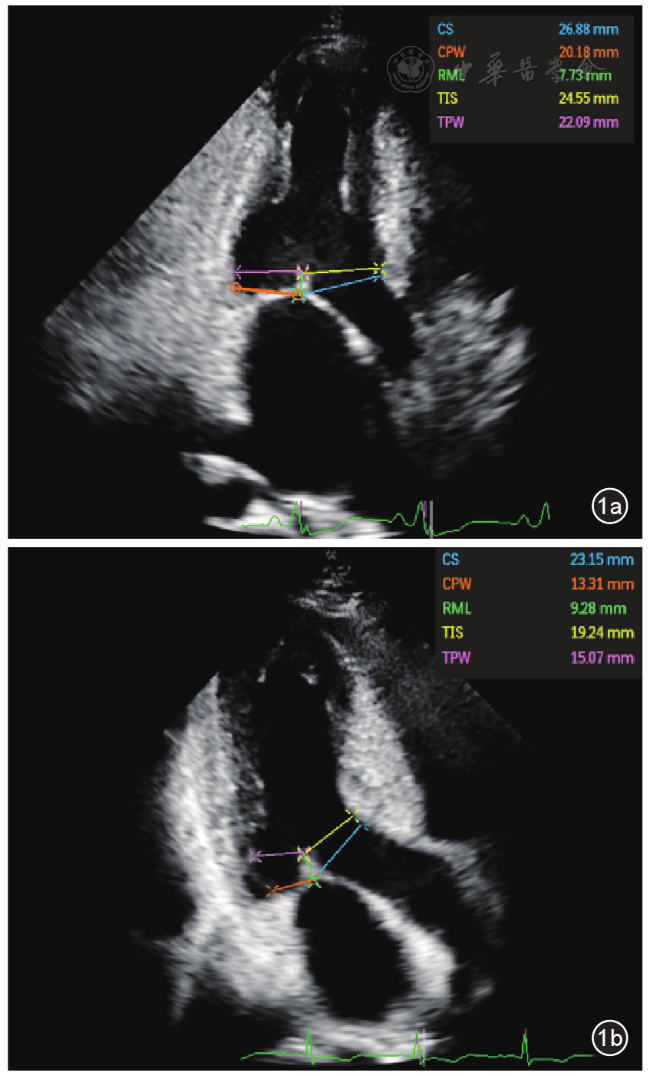
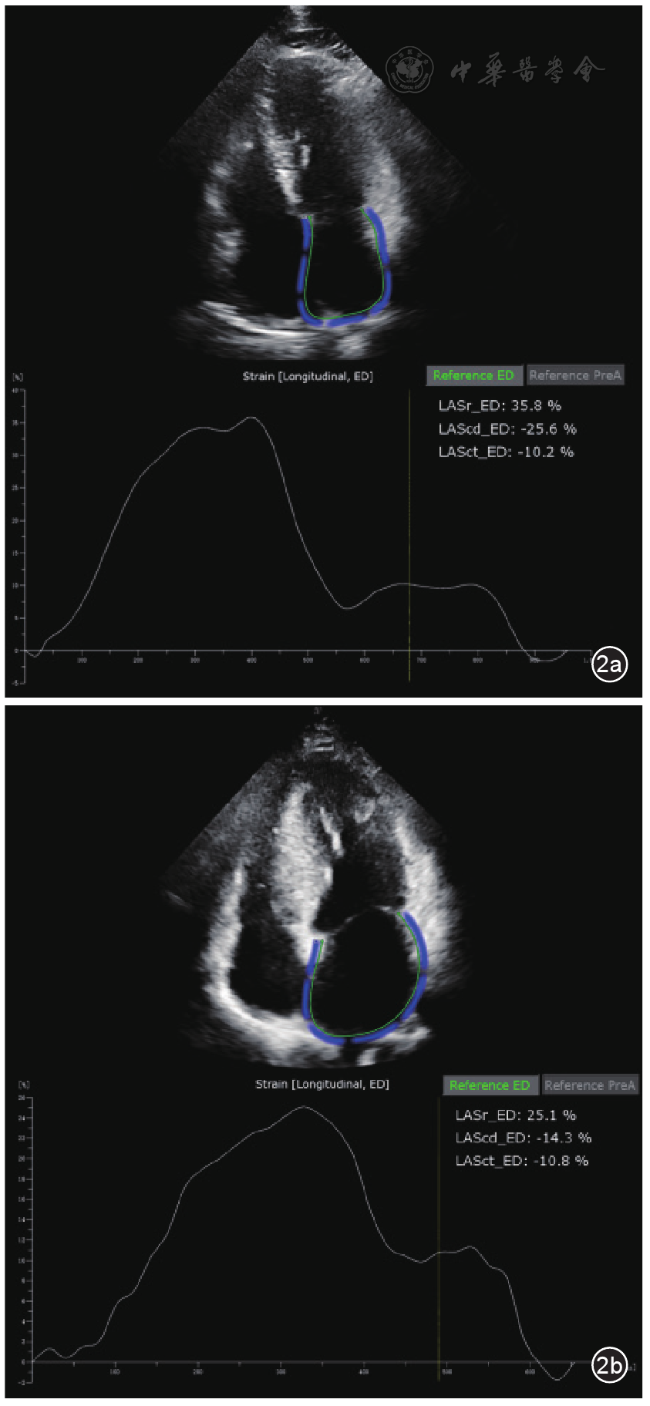
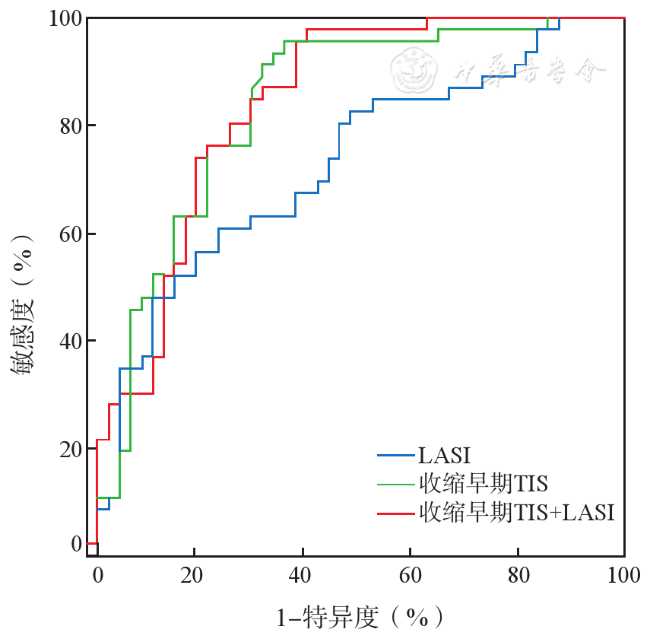
与非梗阻性HCM组相比,静息状态下梗阻性HCM组的舒张期二尖瓣前叶(AML)长度、收缩早期和收缩末期二尖瓣叶剩余长度(RML)、左心房僵硬度指数(LASI)均增大,收缩早期和收缩末期二尖瓣对合点与室间隔的距离(CS)及二尖瓣瓣尖与室间隔的距离(TIS)、左心房储备期应变(LASr)、左心房通道期应变(LAScd)绝对值均减小。HCM患者收缩早期TIS < 21.84 mm、LASI > 0.56是发生LVOTO的独立预测因素,OR值分别为25.248、13.524(P均< 0.05)。收缩早期TIS、LASI及二者联合参数预测HCM合并LVOTO的曲线下面积分别为0.821、0.715、0.827(P均< 0.001),其敏感度分别为95.6%、60.5%、97.8%,特异度分别为63.8%、78.7%、59.2%。收缩早期TIS≥21.84 mm联合LASI≤0.56可排除HCM合并LVOTO或隐匿LVOTO的可能性,其阴性预测值分别为91.3%、95.5%。
静息超声心动图评估的收缩早期TIS、LASI可作为HCM合并LVOTO的独立预测因素。二者的联合应用可实现对HCM合并LVOTO的早期预测,提示进一步实施负荷超声心动图的必要性,使HCM患者的诊疗流程更加合理化。
夏靖涵 , 林凤娇 , 王胰 , 丁戈琦 , 张清凤 , 张红梅 , 谢盛华 , 李明星 , 尹立雪 , 李文华 . 二尖瓣空间变化联合左心房应变对肥厚型心肌病合并左心室流出道梗阻的预测价值[J]. 中华医学超声杂志(电子版), 2024 , 21(06) : 585 -592 . DOI: 10.3877/cma.j.issn.1672-6448.2024.06.006
To evaluate the value of mitral valve spatial parameters combined with left atrial strain parameters assessed by resting echocardiography in predicting left ventricular outflow tract obstruction (LVOTO) in patients with hypertrophic cardiomyopathy (HCM).
Ninety-five patients diagnosed with HCM by echocardiography during outpatient or inpatient visits at the Sichuan Provincial People's Hospital from January 2021 to December 2023 were retrospectively included. Clinical data, conventional echocardiographic parameters, mitral valve spatial parameters, and left atrial strain parameters were obtained. According to left ventricular outflow tract gradient (LVOTG) at rest and after provocation, the subjects were divided into either a non-obstructive HCM group (n=49) or an obstructive HCM group (n=46), and the differences of the above parameters were compared between the two groups. Receiver operating characteristics (ROC) curve analysis was performed on mitral valve parameters and left atrial parameters with statistically significant differences between the two groups in the univariate analysis, and the area under the ROC curve (AUC) was calculated to obtain the optimal cutoff value and sensitivity and specificity. Parameters with statistically significant differences in the ROC curve analysis were subjected to multivariate Logistic regression analysis to identify the independent predictors and evaluate their predictive efficacy for HCM with LVOTO.
Compared with the non-obstructive HCM group, diastolic anterior mitral leaflet (AML), early-systolic and late-systolic residual mitral leaflet (RML), and left atrial stiffness index (LASI) at rest increased in the obstructive HCM group, while early-systolic and late-systolic coaptation point-interventricular septum (CS), early-systolic and late-systolic mitral leaflet tip-interventricular septum (TIS), left atrial strain during reservoir phase (LASr), and the absolute value of left atrial strain during conduit phase(LAScd) decreased. Early-systolic TIS < 21.84 mm and LASI > 0.56 were independent predictors of HCM with LVOTO, with odds ratio values of 25.248 and 13.524, respectively (both P < 0.05). The AUC values of early-systolic TIS, LASI, and their combination were 0.821, 0.715, and 0.827, respectively (all P < 0.001); their sensitivities for predicting HCM with LVOTO were 95.6%, 60.5%, and 97.8%, respectively, and the corresponding specificities were 63.8%, 78.7%, and 59.2%. Early-systolic TIS≥21.84 mm combined with LASI≤0.56 could exclude the possibility of HCM with LVOTO or occult LVOTO, with negative predictive values of 91.3% and 95.5%, respectively.
Early-systolic TIS and LASI assessed by resting echocardiography can serve as independent predictors of LVOTO in HCM. The combined application of the above two parameters can realize early prediction of LVOTO in HCM, suggesting the necessity of stress echocardiography in making the diagnosis and treatment of HCM patients more reasonable.
 ±s表示,两组间比较采用独立样本t检验;不服从正态分布者以M(P25,P75)表示,两组间比较采用Mann-Whitney U检验。计数资料以例(%)表示,两组间比较采用χ 2检验或Fisher确切概率法。应用ROC曲线评价二尖瓣空间参数和左心房应变参数对HCM合并LVOTO的预测效能,计算曲线下面积(area under the curve,AUC),获得最佳截断值及其敏感度和特异度。采用多因素Logistic回归分析HCM合并LVOTO的独立预测因素。观察者内及观察者间的一致性分析采用组内相关系数(intraclass correlation coefficient,ICC)评价。以P < 0.05为差异具有统计学意义。
±s表示,两组间比较采用独立样本t检验;不服从正态分布者以M(P25,P75)表示,两组间比较采用Mann-Whitney U检验。计数资料以例(%)表示,两组间比较采用χ 2检验或Fisher确切概率法。应用ROC曲线评价二尖瓣空间参数和左心房应变参数对HCM合并LVOTO的预测效能,计算曲线下面积(area under the curve,AUC),获得最佳截断值及其敏感度和特异度。采用多因素Logistic回归分析HCM合并LVOTO的独立预测因素。观察者内及观察者间的一致性分析采用组内相关系数(intraclass correlation coefficient,ICC)评价。以P < 0.05为差异具有统计学意义。表1 非梗阻性HCM组与梗阻性HCM组的一般临床资料和常规超声心动图参数比较 |
| 临床资料 | 非梗阻性HCM组(n=49) | 梗阻性HCM组(n=46) | 统计值 | P值 |
|---|---|---|---|---|
| 男性[例(%)] | 33(67.3) | 22(47.8) | χ 2 = 3.709 | 0.054 |
| 年龄[岁,M(P25,P75)] | 46(31,57) | 48(42,58) | Z = -1.288 | 0.198 |
| HR[次/min,M(P25,P75)] | 70(60,76) | 70(64,79) | Z = -1.170 | 0.242 |
| BSA[m2,M(P25,P75)] | 1.78(1.53,1.84) | 1.69(1.60,1.83) | Z = -0.137 | 0.891 |
收缩压(mmHg, ±s) ±s) | 128.16±15.52 | 131.23±18.38 | t = -0.831 | 0.408 |
舒张压(mmHg, ±s) ±s) | 72.96±12.79 | 76.97±9.91 | t = -1.591 | 0.115 |
IVSd(mm, ±s) ±s) | 21.99±5.67 | 22.87±6.67 | t = -0.713 | 0.478 |
| E/e'[M(P25,P75)] | 9.82(7.76,12.93) | 15.25(11.19,18.88) | Z = -4.264 | < 0.001 |
| E/A[M(P25,P75)] | 1.08(0.71,1.44) | 0.97(0.73,1.27) | Z = -0.290 | 0.771 |
LVEF(%, ±s) ±s) | 62.00±8.89 | 58.47±7.09 | t = 2.195 | 0.030 |
| 静息时LVOTG[mmHg,M(P25,P75)] | 5.58(3.40,8.91) | 49.00(22.58,77.11) | Z = -7.678 | < 0.001 |
LVOTd(mm, ±s) ±s) | 12.65±3.16 | 12.26±2.47 | t = 0.657 | 0.513 |
| MR[例(%)] | 18(36.7) | 34(73.9) | χ 2 = 13.237 | < 0.001 |
注:1 mmHg=0.133 kPa;HCM为肥厚型心肌病;HR为心率;BSA为体表面积;IVSd为舒张末期室间隔厚度;E为舒张早期二尖瓣血流速度峰值;A为舒张末期二尖瓣血流速度峰值;e'为间隔侧及侧壁侧二尖瓣环舒张早期运动速度平均峰值;LVEF为左心室射血分数;LVOTG为左心室流出道压力阶差;LVOTd为收缩末期左心室流出道内径;MR为二尖瓣反流 |
表2 非梗阻性HCM组与梗阻性HCM组的二尖瓣空间参数比较 |
| 二尖瓣空间参数 | 非梗阻性HCM组(n=49) | 梗阻性HCM组(n=46) | 统计值 | P值 |
|---|---|---|---|---|
AML(mm, ±s) ±s) | 28.86±2.97 | 30.19±3.00 | t = -2.212 | 0.029 |
| PML[mm,M(P25,P75)] | 14.63(12.96,15.88) | 13.62(12.58,14.94) | Z = -1.913 | 0.056 |
CS(mm, ±s) ±s) | ||||
| 收缩早期 | 25.45±4.46 | 21.01±3.32 | t = 5.516 | < 0.001 |
| 收缩末期 | 20.27±4.29 | 16.35±3.55 | t = 4.823 | < 0.001 |
| CPW(mm) | ||||
收缩早期( ±s) ±s) | 16.20±4.78 | 15.85±4.77 | t = 0.360 | 0.719 |
| 收缩末期[M(P25,P75)] | 12.67(9.85,14.79) | 12.01(9.77,15.17) | Z = -0.220 | 0.826 |
| RML(mm) | ||||
| 收缩早期[M(P25,P75)] | 6.54(5.76,7.62) | 7.75(6.53,9.63) | Z = -3.366 | < 0.001 |
收缩末期( ±s) ±s) | 7.70±1.63 | 8.85±2.14 | t = -2.925 | 0.004 |
| TIS[mm,M(P25,P75)] | ||||
| 收缩早期 | 23.09(19.47,27.50) | 17.93(16.08,19.54) | Z = -5.388 | < 0.001 |
| 收缩末期 | 15.32(13.57,19.61) | 12.22(11.07,14.07) | Z = -4.284 | < 0.001 |
TPW(mm, ±s) ±s) | ||||
| 收缩早期 | 16.84±4.80 | 17.40±4.91 | t = -0.561 | 0.576 |
| 收缩末期 | 12.37±5.52 | 12.38±4.65 | t = -0.014 | 0.989 |
注:HCM为肥厚型心肌病;AML为二尖瓣前叶;PML为二尖瓣后叶;CS为二尖瓣对合点与室间隔的距离;CPW为二尖瓣对合点与后壁的距离;RML为二尖瓣叶剩余长度;TIS为二尖瓣瓣尖与室间隔的距离;TPW为二尖瓣瓣尖与后壁的距离 |
表3 非梗阻性HCM组与梗阻性HCM组的左心房应变参数比较 |
| 左心房应变参数 | 非梗阻性HCM组(n=49) | 梗阻性HCM组(n=46) | 统计值 | P值 |
|---|---|---|---|---|
| LAVImax [ml/m2,M(P25,P75)] | 32.12(22.11,40.11) | 32.83(24.81,43.72) | Z = -0.558 | 0.577 |
LASr(%, ±s) ±s) | 28.33±11.74 | 23.29±9.67 | t = 2.353 | 0.021 |
| LAScd [%,M(P25,P75)] | -14.96(-21.44,-10.16) | -11.81(-13.60,-7.95) | Z = -2.530 | 0.011 |
| LASct [%,M(P25,P75)] | -10.75(-15.62,-7.54) | -11.18(-13.81,-7.00) | Z = -0.489 | 0.625 |
| LASI [M(P25,P75)] | 0.34(0.28,0.59) | 0.70(0.38,1.19) | Z = -4.014 | < 0.001 |
注:HCM为肥厚型心肌病;LAVImax为左心房最大容积指数;LASr为左心房储备期应变;LAScd为左心房通道期应变;LASct为左心房收缩期应变;LASI为左心房僵硬度指数 |
表4 预测HCM合并LVOTO的因素赋值表 |
| 因素 | 赋值 |
|---|---|
| 收缩早期CS | ≥24.77 mm=0,< 24.77 mm=1 |
| 收缩末期CS | ≥18.03 mm=0,< 18.03 mm=1 |
| 收缩早期RML | ≤7.17 mm=0,> 7.17 mm=1 |
| 收缩末期RML | ≤8.18 mm=0,> 8.18 mm=1 |
| 收缩早期TIS | ≥21.84 mm=0,< 21.84 mm=1 |
| 收缩末期TIS | ≥13.57 mm=0,< 13.57 mm=1 |
| LASI | ≤0.56=0,> 0.56=1 |
| LASr | < 27.94%=0,≥27.94%=1 |
| LAScd | ≤-13.84%=0,> -13.84%=1 |
注:CS为二尖瓣对合点与室间隔的距离;RML为二尖瓣叶剩余长度;TIS为二尖瓣瓣尖与室间隔的距离;LASI为左心房僵硬度指数;LASr为左心房储备期应变;LAScd为左心房通道期应变;HCM为肥厚型心肌病;LVOTO为左心室流出道梗阻 |
表5 静息超声心动图参数预测HCM合并LVOTO的多因素Logistic回归分析 |
| 因素 | B值 | SE值 | Wald χ 2值 | OR值(95%CI) | P值 |
|---|---|---|---|---|---|
| 收缩早期CS < 24.77 mm | 0.093 | 1.102 | 0.007 | 1.097(0.126~9.517) | 0.933 |
| 收缩末期CS < 18.03 mm | 0.922 | 0.929 | 0.985 | 2.514(0.407~15.523) | 0.321 |
| 收缩早期RML > 7.17 mm | 0.410 | 0.844 | 0.236 | 1.506(0.288~7.878) | 0.627 |
| 收缩末期RML > 8.18 mm | 1.340 | 0.805 | 2.773 | 3.820(0.789~18.503) | 0.096 |
| 收缩早期TIS < 21.84 mm | 3.229 | 1.265 | 6.517 | 25.248(2.117~301.165) | 0.011 |
| 收缩末期TIS < 13.57 mm | 0.353 | 0.841 | 0.177 | 1.424(0.274~7.403) | 0.674 |
| LASI > 0.56 | 2.604 | 1.034 | 6.342 | 13.524(1.781~102.667) | 0.012 |
| LASr≥27.94% | -0.521 | 0.903 | 0.333 | 0.594(0.101~3.488) | 0.564 |
| LAScd > -13.84% | 0.724 | 0.956 | 0.573 | 2.062(0.317~13.427) | 0.449 |
注:CS为二尖瓣对合点与室间隔的距离;RML为二尖瓣叶剩余长度;TIS为二尖瓣瓣尖与室间隔的距离;LASI为左心房僵硬度指数;LASr为左心房储备期应变;LAScd为左心房通道期应变;HCM为肥厚型心肌病;LVOTO为左心室流出道梗阻 |
| 1 |
刘丽文, 李静, 鲁孝楠, 等. 梗阻性肥厚型心肌病的治疗新进展 [J/OL]. 中华医学超声杂志(电子版), 2021, 18(1): 4-7.
|
| 2 |
张运, 尹立雪, 邓又斌, 等. 负荷超声心动图规范化操作指南 [J]. 中国医学影像技术, 2017, 33(4): 632-638.
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
夏靖涵, 尹立雪, 李明星, 等. 斑点追踪超声心动图在肥厚型心肌病不良心血管事件风险评估中的应用进展 [J/OL]. 中华医学超声杂志(电子版), 2023, 20(12): 1312-1316.
|
| 7 |
|
| 8 |
|
| 9 |
朱峰. 《中国成人肥厚型心肌病诊断与治疗指南2023》要点解读 [J]. 临床心血管病杂志, 2023, 39(6): 413-416.
|
| 10 |
唐璐, 周年伟, 蒋英英, 等. 肥厚型心肌病的基因型与表型分析 [J]. 中华超声影像学杂志, 2020, 29(3): 219-223.
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
李慕子, 李慧, 孟红, 等. 实时三维超声心动图自动定量技术评价肥厚型心肌病患者左心房容积及功能的应用价值 [J]. 中国循环杂志, 2022, 37(5): 487-493.
|
| 17 |
|
| 18 |
|
| 19 |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}