
2024 , Vol. 21 >Issue 10: 943 - 949
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2024.10.003
超声心动图在多发性骨髓瘤心脏淀粉样变中的诊断价值
Copy editor: 汪荣
收稿日期: 2024-09-03
网络出版日期: 2024-12-23
版权
Diagnostic value of echocardiography in cardiac amyloidosis in multiple myeloma
Received date: 2024-09-03
Online published: 2024-12-23
Copyright
目的
探讨超声心动图在多发性骨髓瘤(MM)合并心脏淀粉样变(CA)中的诊断价值。
方法
选取2015年1月至2024年6月于南京鼓楼医院确诊为MM并具有完整超声心动图资料者共93例,其中单纯MM者61例为对照组,MM合并CA者32例为病例组。比较2组患者的超声心动图常规参数及应变参数;采用单因素Logistic回归分析MM合并CA的超声心动图相关参数;采用Pearson分析评价病例组血清脑钠肽(BNP)与超声心动图参数的相关性。
结果
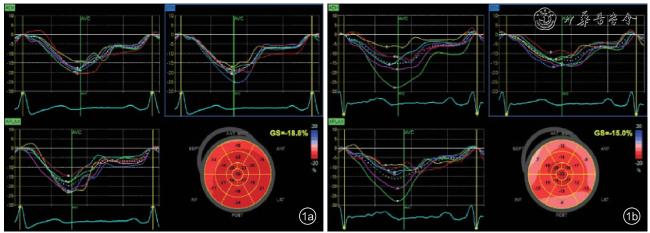
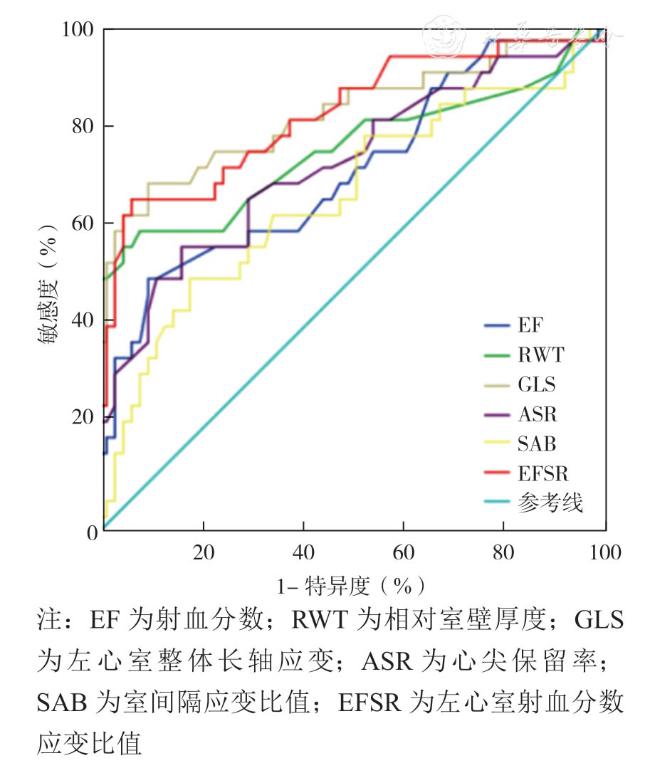
与对照组相比,病例组的超声心动图参数左心房内径(LAD)、左心室室壁厚度、相对室壁厚度(RWT)、E/e'、心尖保留率(ASR)、室间隔应变比值(SAB)及左心室射血分数应变比值(EFSR)均较高,左心室射血分数(LVEF)及左心室整体纵向应变(GLS)较低,差异均具有统计学意义(P均<0.05)。单因素Logistic回归分析显示,LAD、左心室室壁厚度、RWT、E/e'、LVEF、GLS、ASR、SAB及EFSR是评估MM是否合并CA的相关因素,单因素分析结果有统计学意义(P均<0.05)。ROC曲线结果显示,RWT、LVEF、GLS、ASR、SAB及EFSR参数预测MM合并CA的ROC曲线下面积分别为0.754、0.709、0.824、0.724、0.661及0.821(P均<0.05),特异度为82.0% ~ 95.1%,敏感度为50.0%~68.8%,其中GLS与EFSR的预测效能优于其他参数。与对照组相比,病例组血清BNP水平较高(P=0.007);对照组心电图提示肢体导联低电压和(或)V1~V3导联R波递增不良者2例,病例组中15例,差异有统计学意义(P<0.001)。相关性分析显示,病例组中LVEF与血清BNP呈负相关(P<0.001),应变参数GLS、ASR、SAB、EFSR均与血清BNP呈正相关(r = 0.666、0.633、0.396、0.609,P均<0.05)。
结论
超声心动图可以评估MM合并CA的心脏功能受损程度,对预测MM合并CA具有一定的诊断价值,尤其应变参数GLS和EFSR,可以提高对MM合并CA的早期诊断效能,为临床诊疗提供更可靠的依据。
陈慧 , 姚静 , 张宁 , 刘磊 , 马秀玲 , 王小贤 , 方爱娟 , 管静静 . 超声心动图在多发性骨髓瘤心脏淀粉样变中的诊断价值[J]. 中华医学超声杂志(电子版), 2024 , 21(10) : 943 -949 . DOI: 10.3877/cma.j.issn.1672-6448.2024.10.003
Objective
To preliminarily investigate the diagnostic value of echocardiography in multiple myeloma (MM) combined with cardiac amyloidosis (CA) by analyzing echocardiographic parameters retrospectively, in order to provide a clinical basis for early diagnosis of MM combined with CA.
Methods
A total of 93 patients who were diagnosed with MM from January 2015 to June 2024 at Nanjing Drum Tower Hospital and had complete echocardiographic data were selected, including 61 cases with MM alone (control group) and 32 cases with MM combined with CA (case group). Routine echocardiographic parameters and echocardiographic strain parameters were compared between the two groups. Echocardiographic parameters of MM combined with CA were assessed using univariate Logistic regression analysis, and the correlation between serum brain natriuretic peptide (BNP) and echocardiographic parameters in the case group was evaluated using Pearson's analysis.
Results
Compared with the control group, the echocardiographic parameters left atrial diameter (LAD), left ventricular wall thickness, relative ventricular wall thickness (RWT),E/e', apical sparing ratio (ASR), septal apical-septal basal ratio (SAB), and left ventricular ejection fractionto-strain ratio (EFSR) were significantly higher in the case group, and the left ventricular ejection fraction(LVEF) and left ventricular global longitudinal strain (GLS) were significantly lower in the case group (P<0.05 for all).Univariate Logistic regression analysis showed that LAD, left ventricular wall thickness, RWT, E/e',LVEF, GLS, ASR, SAB, and EFSR were factors significantly associated with CA in MM (P<0.05 for all).Receiver operating characteristic (ROC) curve analysis showed that the area under the ROC curve values of RWT, LVEF, GLS, ASR SAB, and EFSR parameters for predicting MM combined with CA were 0.754,0.709, 0.824, 0.724, 0.66, and 0.821, respectively (P<0.05), their specificity ranged from 82.0% to 95.1%,and their sensitivity ranged from 50.0% to 68.8%, with the predictive efficacy of GLS and EFSR being better than that of other parameters. Compared with the control group, serum BNP level was significantly higher in the case group (P=0.007). There were two cases of electrocardiograms suggesting low voltage in limb leads and/or poor R-wave increment in leads V1~V3 in the control group, and 15 cases in the case group, with a statistically significant difference between the two groups (P<0.001). Correlation analysis showed that LVEF was negatively correlated with serum BNP in the case group (P<0.001), and the strain parameters GLS, ASR, SAB, and EFSR were positively correlated with serum BNP (r = 0.666, 0.633, 0.396, and 0.609,respectively; P<0.05 for all).
Conclusion
Echocardiography can be used to assess the degree of cardiac function impairment in MM combined with CA and has appreciated diagnostic value in predicting this condition, especially the strain parameters GLS and EFSR, which can improve the early diagnostic efficacy of MM combined with CA and provide a more reliable basis for clinical diagnosis and treatment.
Key words: Multiple myeloma; Cardiac amyloidosis; Echocardiography
 表示,组间比较采用单因素方差分析;不符合正态分布的计量资料以M(P25,P75)表示,组间比较采用非参数检验。计数资料以例(%)表示。采用单因素Logistic回归分析MM与MM合并CA存在差异的超声心动图参数。绘制ROC曲线分析超声心动图参数对MM合并CA的诊断效能。超声心动图参数与血清脑钠肽之间的相关性分析采用Pearson分析。以P<0.05为差异有统计学意义。
表示,组间比较采用单因素方差分析;不符合正态分布的计量资料以M(P25,P75)表示,组间比较采用非参数检验。计数资料以例(%)表示。采用单因素Logistic回归分析MM与MM合并CA存在差异的超声心动图参数。绘制ROC曲线分析超声心动图参数对MM合并CA的诊断效能。超声心动图参数与血清脑钠肽之间的相关性分析采用Pearson分析。以P<0.05为差异有统计学意义。表1 病例组与对照组基线资料比较 |
| 组别 | 例数 | 年龄(岁,±s) | 性别[男性,例(%)] | BMI(kg/m2,±s) | 血清BNP[pg/ml,M(P25,P75)] | 心电图改变[例(%)] |
|---|---|---|---|---|---|---|
| 对照组 | 61 | 63.08±10.38 | 32(52.50) | 23.18±3.33 | 47.10(23.40,100.50) | 2(3.30) |
| 病例组 | 32 | 59.94±11.06 | 22(68.70) | 22.96±2.89 | 313.00(78.95,565.75) | 15(46.90) |
| 统计值 | t=1.330 | χ2=2.228 | t=0.306 | Z=-3.950 | χ2=26.705 | |
| P值 | 0.189 | 0.130 | 0.760 | 0.007 | <0.001 |
表2 病例组与对照组超声心动图常规参数比较( |
| 组别 | 例数 | LVDd(mm) | LVDs(mm) | LAD(mm) | IVSTd(mm) | LVPWTd(mm) | RWT | E/e' | LVEF(%) |
|---|---|---|---|---|---|---|---|---|---|
| 对照组 | 61 | 48.98±4.14 | 32.70±3.13 | 37.08±4.56 | 9.14±1.31 | 9.01±1.15 | 0.37±0.05 | 9.93±3.19 | 61.74±2.63 |
| 病例组 | 32 | 47.41±3.64 | 32.82±3.15 | 39.91±5.68 | 11.79±3.27 | 11.37±2.69 | 0.48±0.13 | 17.88±8.81 | 58.21±5.83 |
| t值 | 1.815 | -0.169 | 0.335 | -5.545 | -5.932 | -6.187 | -6.322 | 4.021 | |
| P值 | 0.073 | 0.866 | 0.011 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
表3 病例组与对照组超声心动图应变参数比较( |
| 组别 | 例数 | GLS | ASR | SAB | EFSR |
|---|---|---|---|---|---|
| 对照组 | 61 | -19.18±2.56 | 0.63±0.11 | 1.97±0.98 | 3.27±0.43 |
| 病例组 | 32 | -14.51±4.50 | 0.78±0.25 | 3.56±2.73 | 4.39±1.36 |
| t值 | -6.381 | -4.218 | -2.118 | -5.904 | |
| P值 | <0.001 | <0.001 | 0.037 | <0.001 |
表4 超声心动图参数单因素Logistic回归分析 |
| 参数 | β | E | Wald | 自由度 | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|---|
| LVDd | -0.108 | 0.061 | 3.314 | 1 | 0.077 | 0.897 | 0.796~1.102 |
| LAD | 0.115 | 0.047 | 5.898 | 1 | 0.015 | 1.122 | 1.022~1.231 |
| IVSTd | 0.546 | 0.133 | 16.954 | 1 | <0.001 | 1.726 | 1.331~2.239 |
| LVPWTd | 0.642 | 0.151 | 18.205 | 1 | <0.001 | 1.901 | 1.415~2.553 |
| RWT | 14.703 | 3.475 | 17.907 | 1 | <0.001 | 2429356 | 2678.8~2.2×109 |
| E/e' | 0.207 | 0.047 | 19.233 | 1 | <0.001 | 1.230 | 1.121~1.350 |
| LVEF | -0.253 | 0.083 | 9.295 | 1 | 0.002 | 0.777 | 0.660~0.914 |
| GLS | 0.440 | 0.105 | 17.606 | 1 | <0.001 | 1.552 | 1.264~1.906 |
| ASR | 6.401 | 1.936 | 10.927 | 1 | 0.001 | 602.376 | 13.540~26798 |
| SAB | 0.432 | 0.199 | 4.735 | 1 | 0.030 | 1.541 | 1.044~2.274 |
| EFSR | 2.200 | 0.581 | 14.318 | 1 | <0.001 | 9.028 | 2.888~28.220 |
表5 超声心动图相关参数诊断MM合并CA的效能分析 |
| 参数 | 截断值 | 敏感度(%) | 特异度(%) | ROC曲线下面积 | P值 | 95%CI |
|---|---|---|---|---|---|---|
| LVEF | 59.5% | 50.0 | 90.1 | 0.709 | 0.001 | 0.593~0.825 |
| RWT | 0.46 | 56.3 | 95.1 | 0.754 | <0.001 | 0.635~0.874 |
| GLS | -16.4% | 68.8 | 90.2 | 0.824 | <0.001 | 0.722~0.925 |
| ASR | 0.72 | 56.3 | 83.6 | 0.724 | <0.001 | 0.610~0.839 |
| SAB | 2.34 | 50.0 | 82.0 | 0.661 | 0.011 | 0.538~0.783 |
| EFSR | 3.77 | 65.6 | 93.4 | 0.821 | <0.001 | 0.723~0.919 |
| 1 |
Bergstrom DJ, Kotb R, Louzada ML, et al. Consensus guidelines on the diagnosis of multiple myeloma and related disorders:Recommendations of the Myeloma Canada Research Network Consensus Guideline Consortium[J].Clin Lymphoma Myeloma Leuk,2020, 20(7): e352-e367.
|
| 2 |
Cowan AJ, Green DJ, Kwok M, et al.Diagnosis and management of multiple myeloma: a review[J]. JAMA, 2022, 327(5): 464-477.
|
| 3 |
中国医师协会血液科医师分会, 中华医学会血液学分会. 中国多发性骨髓瘤诊治指南(2022年修订)[J]. 中华内科杂志, 2022, 61(5):480-487.
|
| 4 |
Aljaroudi WA, Desai MY, Tang WH,et al. Role of imaging in the diagnosis and management of patients with cardiac amyloidosis: state of the art review and focus on emerging nuclear techniques[J]. Nucl Cardiol, 2014, 21(2): 271-283.
|
| 5 |
Dorbala S, Cuddy S, Falk RH. How to image cardiac amyloidosis: a practical approach[J]. JACC Cardiovasc Imaging, 2020, 13(6): 1368-1383.
|
| 6 |
关莹, 李越, 温朝阳, 等. 超声心动图联合心电图对心肌淀粉样变的诊断价值[J/CD]. 中华医学超声杂志(电子版), 2011, 8(2): 313-318.
|
| 7 |
Phelan D, Collier P, Thavendiranathan P, et al. Relative apical sparing of longitudinal strain using two-dimensional speckle-tracking echocardiography is both sensitive and specific for the diagnosis of cardiac amyloidosis[J].Heart, 2012, 98(19): 1442-1448.
|
| 8 |
Phelan D, Thavendiranathan P, Popovic Z, et al. Application of a parametric display of two-dimensional speckle-tracking longitudinal strain to improve the etiologic diagnosis of mild to moderate left ventricular hypertrophy[J]. J Am Soc Echocardiogr, 2014, 27(8): 888-895.
|
| 9 |
Radocha J, van de Donk N, Weisel K. Monoclonal antibodies and antibody drug conjugates in multiple myeloma[J]. Cancers (Basel),2021, 13(7): 1571.
|
| 10 |
Moriyama S, Fukata M, Hieda M, et al. Early-onset cardiac dysfunction following allogeneic haematopoietic stem cell transplantation[J]. Open Heart, 2022, 9(1): e002007.
|
| 11 |
Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update [J]. J Clin Oncol, 2020, 38(5): 496-520.
|
| 12 |
Koyama J, Falk RH. Prognostic significance of strain Doppler imaging in light-chain amyloidosis[J]. JACC Cardiovasc Imaging, 2010, 3(4):333-342.
|
| 13 |
Senapati A, Sperry BW, Grodin JL, et al. Prognostic implication of relative regional strain ratio in cardiac amyloidosis[J]. Heart, 2016,102(10): 748-754.
|
| 14 |
Kyrouac D, Schiffer W, Lennep B, et al. Echocardiographic and clinical predictors of cardiac amyloidosis: limitations of apical sparing[J]. ESC Heart Fail, 2022, 9(1): 385-397.
|
| 15 |
Cotella J, Randazzo M, Maurer MS, et al. Limitations of apical sparing pattern in cardiac amyloidosis: a multicentre echocardiographic study[J]. Eur Heart J Cardiovasc Imaging, 2024, 25(6): 754-761.
|
| 16 |
Dorbala S, Ando Y, Bokhari S, et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2-evidence base and standardized methods of imaging[J]. Circ Cardiovasc Imaging, 2021, 14(7): e000029.
|
| 17 |
Pagourelias ED, Duchenne J, Mirea O, et al. The relation of ejection fraction and global longitudinal strain in amyloidosis: implications for differential diagnosis[J]. J Am Coll Cardiol Img, 2016, 9(11): 1358-1359.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}