
2024 , Vol. 21 >Issue 10: 950 - 958
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2024.10.004
胎儿心脏超声定量多参数对主动脉缩窄胎儿心脏结构及功能的诊断价值
Copy editor: 汪荣
收稿日期: 2024-07-03
网络出版日期: 2024-12-23
基金资助
国家重点研发计划项目(2023YFC2705701)浙江大学科学技术研究院一般横向项目(校合-2021-KYY-518053-0055)
版权
Value of multiple fetal echocardiographic quantitative parameters in assessing heart structure and function in fetuses with coarctation of the aorta
Received date: 2024-07-03
Online published: 2024-12-23
Copyright
目的
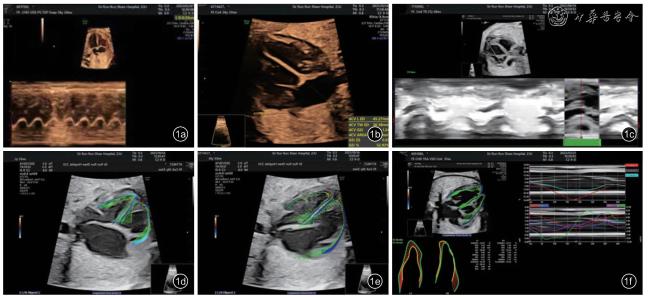
探讨胎儿心脏定量分析(fetal HQ)技术联合其他胎儿心脏定量多参数在评估主动脉缩窄(CoA)胎儿心脏结构及功能中的应用价值。
方法
选取2022年1月至2023年1月在浙江大学医学院附属邵逸夫医院超声科行胎儿超声心动图检查疑诊CoA的50例胎儿作为研究对象,将分娩后门诊随访确诊为CoA的胎儿纳入CoA组(18例),将门诊随访明确为CoA假阳性的纳入对照组(32例)。比较2组胎儿的整体心血管参数包括左心室面积变化率(LVFAC)、LVFAC Z-评分、左心室整体纵向应变(LVGLS)、右心室整体纵向应变(RVGLS)、右心室面积/左心室面积(RVA/ LVA)、主动脉峡部内径(AI)及其Z评分(AI Z-评分)、主动脉峡部内径/降主动脉内径(AI/DAO)、主肺动脉内径/升主动脉内径(MPA/AAO);比较2组左、右心室24节段的舒张末期横径(ED)、ED Z-评分、短轴缩短率(FS)、FS Z-评分、球形指数(SI)、SI Z-评分。应用多因素Logistic回归分析CoA的独立危险因素;采用ROC曲线分析LVFAC、LVFAC Z-评分、AI及三者联合对胎儿CoA的诊断效能。采用组内相关系数(ICC)判断观察者内及观察者间测量参数的一致性。
结果
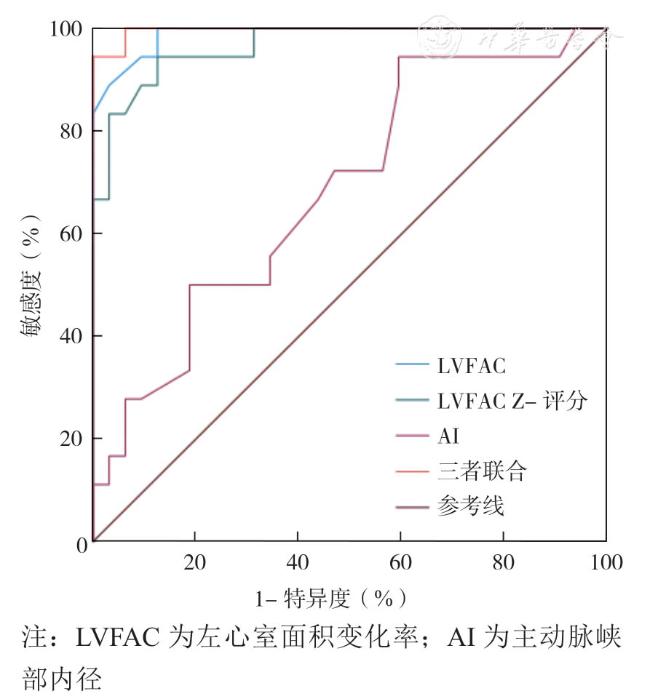
CoA组胎儿的RVA /LVA、MPA/AAO明显高于对照组,LVFAC、LVFAC Z-评分、LVGLS、RVGLS、AI、AI Z-评分、AI/DAO明显低于对照组(P<0.05);CoA组左心室第1节段的ED Z-评分显著低于对照组(P<0.05),左心室第4~8节段的FS、FS Z-评分均显著高于对照组(P<0.05)。LVFAC、LVFAC Z-评分、AI是CoA的独立危险因素(P<0.05);LVFAC、LVFAC Z-评分、AI及三者联合的ROC曲线下面积分别为0.989(0.969 ~ 1.000)、0.966(0.922 ~ 1.000)、0.785(0.731 ~ 0.859)和0.997(0.987 ~ 1.000)。观察者内及观察者间测量胎儿各参数的ICC为0.90~0.99。
结论
fetal HQ联合其他胎儿心脏定量多参数能够有效评估CoA胎儿心脏结构、大小及功能改变,为进一步提高CoA胎儿诊断准确性提供参考信息。
关键词: 胎儿; 主动脉弓缩窄; 胎儿心脏定量分析技术; 超声心动图; 先天性心脏病
戴飞 , 赵博文 , 潘美 , 彭晓慧 , 陈冉 , 田园诗 , 狄敏 . 胎儿心脏超声定量多参数对主动脉缩窄胎儿心脏结构及功能的诊断价值[J]. 中华医学超声杂志(电子版), 2024 , 21(10) : 950 -958 . DOI: 10.3877/cma.j.issn.1672-6448.2024.10.004
Objective
To evaluate the value of fetal heart quantitation (fetal HQ) combined with other multiple fetal echocardiographic quantitative parameters in evaluating heart structure and function in fetuses with coarctation of the aorta (CoA).
Methods
Fifty fetuses suspected of having CoA who underwent fetal echocardiography at the Department of Diagnostic Ultrasound & Echocardiography, Sir Run Run Shaw Hospital, Zhejiang University College of Medicine from January 2022 to January 2023 were selected as the study subjects. The fetuses diagnosed with CoA in the outpatient follow-up after delivery were included in a CoA group (18 cases), and those with false-positive results as demonstrated during outpatient follow-up were included in a control group (32 cases). Overall cardiovascular parameters of the two groups of fetuses were compared, including left ventricular fractional area change (LVFAC), LVFAC Z-score, left ventricular global longitudinal strain (LVGLS), right ventricular global longitudinal strain (RVGLS), right ventricular area (RVA)/left ventricular area (LVA) ratio, aortic isthmus inner diameter (AI) and its Z score (AI Z-score),aortic isthmus inner diameter/descending aorta inner diameter ratio (AI/DAO ratio), main pulmonary artery inner diameter/ascending aorta inner diameter ratio (MPA/AAO ratio). The end diastolic transverse diameter(ED), ED Z-score, short axis shortening rate (FS), FS Z-score, sphericity index (SI), and SI Z-score of the 24 segments of the left and right ventricle were also compared between the two groups. Multivariate Logistic regression analysis was performed to identify risk factors for CoA. Receiver operating characteristics(ROC) curve analysis was performed to test the diagnostic efficacy of LVFAC, LVFAC Z-score, AI, and the combination of the three for fetal CoA. Within-group correlation coefficients (ICCs) were used to judge the consistency of measured parameters within and between observers.
Results
LVFAC, LVFAC Z-score,LVGLS, RVGLS, AI, AI Z-score, and AI/DAO ratio were significantly lower in the CoA group than in the control group, while RVA /LVA ratio and MPA/AAO ratio of fetuses in the CoA group were significantly higher than those of the control group (P<0.05). The ED Z-score of the first segment of the left ventricle in the CoA group was significantly lower than that of the control group (P<0.05), and the FS Z-scores of the fourth to eighth segments of the left ventricle were significantly higher than those of the control group (P<0.05). LVFAC, LVFAC Z-score, and AI were identified to be risk factors for CoA (P<0.05). The area under the ROC curve values of LVFAC, LVFAC Z-score, AI, and their combination for diagnosing fetal CoA were 0.989 (0.969 ~ 1.000), 0.966 (0.922 ~ 1.000), 0.785 (0.731 ~ 0.859), and 0.997 (0.987 ~ 1.000),respectively. The ICCs for intra-observer and inter-observer measurements of various fetal parameters ranged from 0.90 to 0.99.
Conclusion
Fetal HQ combined with other multiple fetal echocardiographic quantitative parameters can effectively evaluate the changes of heart structure, size, and function in fetuses with CoA,providing reference information for improving prenatal detection of CoA.
 表示,2组间比较采用独立样本t检验;应用多因素Logistic回归分析CoA的危险因素;应用受试者工作特征(receiver operating characteristic,ROC)曲线分析LVFAC、LVFAC Z-评分、AI及三者联合对胎儿CoA的诊断效能;采用组内相关系数(intra-group correlation coefficient,ICC)判断观察者内及观察者间测量参数的一致性。以P<0.05为差异有统计学意义。
表示,2组间比较采用独立样本t检验;应用多因素Logistic回归分析CoA的危险因素;应用受试者工作特征(receiver operating characteristic,ROC)曲线分析LVFAC、LVFAC Z-评分、AI及三者联合对胎儿CoA的诊断效能;采用组内相关系数(intra-group correlation coefficient,ICC)判断观察者内及观察者间测量参数的一致性。以P<0.05为差异有统计学意义。表1 CoA组与对照组胎儿整体心血管参数比较( |
| 参数 | CoA组(n=18) | 对照组(n=32) | t值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 31.56±3.94 | 29.75±3.90 | 1.569 | 0.123 |
| 孕龄(周) | 28.39±4.91 | 28.28±3.55 | 0.091 | 0.928 |
| TAPSE(mm) | 7.40±0.86 | 7.09±0.57 | 1.532 | 0.132 |
| 纵径(mm) | 35.92±7.73 | 36.54±6.68 | 0.298 | 0.767 |
| 横径(mm) | 30.83±7.67 | 30.32±5.06 | 0.283 | 0.778 |
| 面积(mm2) | 894.65±418.50 | 891.54±296.56 | 0.031 | 0.976 |
| 面积Z评分 | 0.02±1.15 | 0.05±1.16 | 0.088 | 0.930 |
| GSI | 1.18±0.12 | 1.21±0.13 | 0.805 | 0.425 |
| SI Z评分 | -0.53±1.18 | -0.20±1.30 | 0.890 | 0.378 |
| EF(%) | 57.67±9.64 | 53.56±5.59 | 1.914 | 0.061 |
| EF Z-评分 | -0.63±1.44 | -1.22±0.80 | 1.869 | 0.068 |
| LVFAC(%) | 35.82±2.90 | 44.94±2.68 | -11.20 | <0.001 |
| LVFAC Z-评分 | -0.48±1.51 | -1.19±0.81 | -8.955 | <0.001 |
| CO(mL/min) | 103.21±96.62 | 103.56±51.58 | 0.017 | 0.987 |
| CO Z-评分 | -0.70±1.53 | -0.91±0.70 | 0.666 | 0.509 |
| LVGLS(%) | 20.91±3.69 | 23.66±4.42 | 2.235 | 0.030 |
| RVFAC(%) | 35.82±10.93 | 37.59±4.85 | 0.792 | 0.432 |
| RVFAC Z-评分 | -1.14±2.15 | -0.78±1.13 | 0.779 | 0.440 |
| RVGLS(%) | 20.87±3.40 | 22.72±2.32 | 2.282 | 0.027 |
| RVW/LVW | 1.51±0.39 | 1.38±0.26 | 1.413 | 0.164 |
| RVL/LVL | 0.01±0.02 | 0.01±0.03 | 0.000 | 1.000 |
| RVA/LVA | 1.76±0.77 | 1.38±0.44 | 2.228 | 0.030 |
| AO | 3.72±1.08 | 3.87±1.08 | 0.471 | 0.639 |
| AO Z-评分 | -1.71±1.61 | -1.31±1.48 | 0.889 | 0.378 |
| AAO(mm) | 3.95±1.31 | 4.13±0.94 | 0.563 | 0.576 |
| AAO Z-评分 | -2.41±1.72 | -1.86±1.32 | 1.266 | 0.211 |
| AI(mm) | 1.88±0.51 | 2.24±0.58 | 2.197 | 0.033 |
| AI Z-评分 | -4.32±1.12 | -3.30±1.10 | 3.127 | 0.003 |
| AI/AAO | 0.48±0.15 | 0.54±0.09 | 1.773 | 0.083 |
| AI/DAO | 0.43±0.09 | 0.59±0.12 | 4.923 | <0.001 |
| AI/AO | 0.53±0.15 | 0.59±0.10 | 1.695 | 0.096 |
| MPA/AAO | 1.79±0.31 | 1.57±0.34 | 2.265 | 0.028 |
表2 CoA组与对照组胎儿左心室24节段ED Z-评分比较( |
| 组别 | 例数 | EDZ1 | EDZ2 | EDZ3 | EDZ4 | EDZ5 | EDZ6 | EDZ7 | EDZ8 |
|---|---|---|---|---|---|---|---|---|---|
| CoA组 | 18 | -0.77±1.17 | -0.61±1.19 | -0.44±1.25 | -0.28±1.33 | -0.23±1.27 | -0.18±1.34 | -0.17±1.41 | -0.21±1.49 |
| 对照组 | 32 | -0.06±1.15 | -0.03±1.10 | 0.02±1.06 | 0.05±1.02 | 0.04±0.93 | 0.03±0.96 | 0.00±0.98 | -0.05±1.01 |
| t值 | 2.083 | 1.738 | 1.381 | 0.983 | 0.862 | 0.642 | 0.501 | 0.452 | |
| P值 | 0.043 | 0.088 | 0.174 | 0.330 | 0.393 | 0.524 | 0.618 | 0.653 | |
| 组别 | 例数 | EDZ9 | EDZ10 | EDZ11 | EDZ12 | EDZ13 | EDZ14 | EDZ15 | EDZ16 |
| CoA组 | 18 | -0.28±1.56 | -0.38±1.61 | -0.48±1.65 | -0.57±1.68 | -0.63±1.70 | -0.64±1.70 | -0.64±1.70 | -0.66±1.68 |
| 对照组 | 32 | -0.11±1.02 | -0.17±1.01 | -0.22±0.99 | -0.28±0.96 | -0.34±0.92 | -0.41±0.87 | -0.50±0.83 | -0.59±0.81 |
| t值 | 0.466 | 0.568 | 0.698 | 0.779 | 0.786 | 0.635 | 0.392 | 0.199 | |
| P值 | 0.643 | 0.573 | 0.488 | 0.439 | 0.436 | 0.529 | 0.697 | 0.843 | |
| 组别 | 例数 | EDZ17 | EDZ18 | EDZ19 | EDZ20 | EDZ21 | EDZ22 | EDZ23 | EDZ24 |
| CoA组 | 18 | -0.73±1.67 | -0.87±1.65 | -1.05±1.62 | -1.19±1.54 | -1.27±1.44 | -1.31±1.37 | -1.32±1.33 | -1.33±1.30 |
| 对照组 | 32 | -0.71±0.83 | -0.87±0.89 | -1.02±0.99 | -1.13±1.08 | -1.17±1.15 | -1.19±1.18 | -1.19±1.20 | -1.19±1.21 |
| t值 | 0.057 | 0.000 | 0.081 | 0.161 | 0.269 | 0.326 | 0.354 | 0.382 | |
| P值 | 0.955 | 1.000 | 0.935 | 0.872 | 0.789 | 0.746 | 0.725 | 0.704 |
表3 CoA组与对照组胎儿左心室24节段FS比较( |
| 组别 | 例数 | FS1 | FS2 | FS3 | FS4 | FS5 | FS6 | FS7 | FS8 |
|---|---|---|---|---|---|---|---|---|---|
| CoA组 | 18 | 15.01±12.94 | 17.68±10.29 | 20.08±9.19 | 22.22±9.26 | 24.09±9.56 | 25.71±9.53 | 27.05±9.35 | 28.03±9.31 |
| 对照组 | 32 | 12.90±11.01 | 14.31±9.30 | 15.63±8.11 | 16.92±7.43 | 18.23±7.12 | 19.63±7.02 | 21.08±7.13 | 22.54±7.38 |
| t值 | 0.611 | 1.184 | 1.775 | 2.214 | 2.465 | 2.580 | 2.537 | 2.296 | |
| P值 | 0.544 | 0.242 | 0.082 | 0.032 | 0.017 | 0.013 | 0.014 | 0.026 | |
| 组别 | 例数 | FS9 | FS10 | FS11 | FS12 | FS13 | FS14 | FS15 | FS16 |
| CoA组 | 18 | 28.57±9.39 | 28.59±9.45 | 28.26±9.62 | 27.83±10.08 | 27.59±10.74 | 27.80±11.31 | 28.32±11.76 | 28.91±12.16 |
| 对照组 | 32 | 23.92±7.64 | 25.15±7.86 | 26.23±8.12 | 27.19±8.41 | 28.08±8.58 | 28.93±8.64 | 29.68±8.87 | 30.22±9.39 |
| t值 | 1.901 | 1.381 | 0.794 | 0.240 | 0.177 | 0.397 | 0.462 | 0.425 | |
| P值 | 0.063 | 0.174 | 0.431 | 0.811 | 0.860 | 0.693 | 0.646 | 0.673 | |
| 组别 | 例数 | FS17 | FS18 | FS19 | FS20 | FS21 | FS22 | FS23 | FS24 |
| CoA组 | 18 | 29.34±12.57 | 29.40±13.22 | 29.15±14.49 | 28.72±16.33 | 28.24±18.30 | 27.88±19.83 | 27.64±20.85 | 27.51±21.43 |
| 对照组 | 32 | 30.44±9.99 | 30.27±10.54 | 29.76±11.46 | 29.06±12.94 | 28.36±14.67 | 27.83±16.12 | 27.49±17.13 | 27.29±17.72 |
| t值 | 0.340 | 0.255 | 0.164 | 0.081 | 0.025 | 0.010 | 0.027 | 0.039 | |
| P值 | 0.735 | 0.799 | 0.870 | 0.936 | 0.980 | 0.992 | 0.978 | 0.969 |
表4 CoA组与对照组胎儿左心室24节段FS Z-评分比较( |
| 组别 | 例数 | FSZ1 | FSZ2 | FSZ3 | FSZ4 | FSZ5 | FSZ6 | FSZ7 | FSZ8 |
|---|---|---|---|---|---|---|---|---|---|
| CoA组 | 18 | -0.39±1.54 | -0.15±1.26 | 0.07±1.16 | 0.23±1.21 | 0.37±1.24 | 0.42±1.21 | 0.36±1.22 | 0.21±1.27 |
| 对照组 | 32 | -0.64±1.31 | -0.56±1.14 | -0.49±1.02 | -0.46±0.97 | -0.39±0.92 | -0.35±0.89 | -0.41±0.93 | -0.54±1.01 |
| t值 | 0.608 | 1.175 | 1.774 | 2.207 | 3.217 | 2.575 | 2.508 | 2.295 | |
| P值 | 0.546 | 0.246 | 0.082 | 0.032 | 0.002 | 0.013 | 0.015 | 0.026 | |
| 组别 | 例数 | FSZ9 | FSZ10 | FSZ11 | FSZ12 | FSZ13 | FSZ14 | FSZ15 | FSZ16 |
| CoA组 | 18 | -0.03±1.30 | -0.31±1.28 | -0.60±1.26 | -0.85±1.24 | -1.01±1.24 | -1.09±1.23 | -1.11±1.20 | -1.10±1.17 |
| 对照组 | 32 | -0.67±1.06 | -0.78±1.07 | -0.87±1.06 | -0.93±1.04 | -0.95±0.99 | -0.97±0.94 | -0.97±0.91 | -0.98±0.90 |
| t值 | 1.888 | 1.389 | 0.808 | 0.244 | 0.188 | 0.387 | 0.465 | 0.406 | |
| P值 | 0.065 | 0.171 | 0.423 | 0.809 | 0.852 | 0.700 | 0.644 | 0.687 | |
| 组别 | 例数 | FSZ17 | FSZ18 | FSZ19 | FSZ20 | FSZ21 | FSZ22 | FSZ23 | FSZ24 |
| CoA组 | 18 | -1.12±1.14 | -1.17±1.14 | -1.23±1.18 | -1.32±1.28 | -1.34±1.34 | -1.35±1.39 | -1.35±1.42 | -1.35±1.44 |
| 对照组 | 32 | -1.02±0.91 | -1.10±0.91 | -1.18±0.93 | -1.30±1.01 | -1.33±1.08 | -1.35±1.13 | -1.36±1.16 | -1.37±1.19 |
| t值 | 0.340 | 0.238 | 0.165 | 0.061 | 0.029 | 0.000 | 0.027 | 0.053 | |
| P值 | 0.735 | 0.813 | 0.869 | 0.952 | 0.977 | 1.000 | 0.979 | 0.958 |
表5 多因素Logistic回归分析CoA的独立危险因素 |
| 因素 | β | SE | Wald χ2 | P值 | OR(95%CI) |
| LVFAC | 1.450 | 0.566 | 6.567 | <0.001 | 4.265(1.406~12.928) |
| LVFAC Z-评分 | 1.464 | 0.518 | 7.990 | <0.001 | 4.324(1.566~11.933) |
| LVGLS | 0.506 | 0.527 | 0.923 | 0.415 | 1.659(0.590~4.660) |
| RVGLS | 0.614 | 0.537 | 1.305 | 0.238 | 1.847(0.645~5.294) |
| RVA/LVA | 0.859 | 0.519 | 2.740 | 0.167 | 2.361(0.854~6.529) |
| AI | 1.166 | 0.435 | 7.181 | <0.001 | 3.208(1.368~7.528) |
| AI Z-评分 | 0.758 | 0.421 | 3.242 | 0.106 | 2.134(0.935~4.870) |
| AI/DAO | 0.725 | 0.468 | 2.401 | 0.233 | 2.065(0.825~5.167) |
| MPA/AAO | 0.427 | 0.562 | 0.576 | 0.418 | 1.532(0.509~4.611) |
| 1 |
Salciccioli KB, Zachariah JP. Coarctation of the aorta: modern paradigms across the lifespan[J]. Hypertension, 2023, 80(10): 1970-1979.
|
| 2 |
Sadeghipour P, Mohebbi B, Firouzi A, et al. Balloon-expandable Cheatham-Platinum stents versus self-expandable nitinol stents in coarctation of aorta: a randomized controlled trial[J]. JACC Cardiovasc Interv, 2022, 15(3): 308-317.
|
| 3 |
Tan F, Yang J, Shen Y, et al. Evaluating fetal heart morphology in hypertensive disorders of pregnancy using the fetal heart quantitative technique[J]. Transl Pediatr, 2022, 11(11): 1804-1812.
|
| 4 |
Wang W, Liu JF, Yin H, et al. Evaluation of fetal cardiac function in fetal growth restriction via fetal HQ analysis based on two-dimensional STI[J]. J Obstet Gynaecol Res, 2023, 49(6): 1514- 1524.
|
| 5 |
詹梦娜, 赵博文, 彭晓慧, 等. 胎儿心脏定量分析技术评价左心室流出道梗阻胎儿心脏功能和形态[J]. 中华超声影像学杂志, 2021,31(10): 854-860.
|
| 6 |
Chen Y, Chen Q, Wu Y, et al. Fetal cardiac geometry and function in pregnancies with well-controlled gestational diabetes mellitus using Fetal HQ[J]. J Matern Fetal Neonatal Med, 2022, 35(25): 8331-8337.
|
| 7 |
中华医学会超声医学分会妇产超声学组. 胎儿主动脉缩窄超声检查中国专家共识(2022版)[J]. 中华超声影像学杂志, 2022, 31(3):203-207.
|
| 8 |
Kailin JA, Santos AB, Yilmaz Furtun B, et al. Isolated coarctation of the aorta in the fetus: A diagnostic challenge[J]. Echocardiography,2017, 34(12): 1768-1775.
|
| 9 |
姜玉新, 张运. 超声医学高级教程[M]. 北京: 中华医学电子音像出版社, 2021: 147-148.
|
| 10 |
沈艳, 骆志玲, 孟红, 等. 综合超声心动图指标在诊断胎儿主动脉缩窄中的应用[J/OL]. 中华医学超声杂志(电子版), 2022, 19 (11):1205-1210.
|
| 11 |
Deiros-Bronte L, Diez-Sebastian J, Rodríguez González R, et al.Prenatal diagnosis of aortic coarctation: prediction algorithm according to gestational age[J]. Fetal Diagn Ther, 2021, 48(11-12): 819-828.
|
| 12 |
Wang Y, Liu C, Zhang Y, et al. Prenatal diagnosis of coarctation of the aorta with a long and angled isthmus by two- and three-dimensional echocardiography: a case report[J]. BMC Cardiovasc Disord, 2021,21(1): 176-182.
|
| 13 |
Contro E, Cattani L, Balducci A, et al. Prediction of neonatal coarctation of the aorta at fetal echocardiography: a scoring system[J]. J Matern Fetal Neonatal Med, 2022, 35(22): 4299-4305.
|
| 14 |
Wang HH, Wang XM, Zhu M, et al. A clinical prediction model to estimate the risk for coarctation of the aorta: From fetal to newborn life[J]. J Obstet Gynaecol Res, 2022, 48(9): 2304-2313.
|
| 15 |
Zwanenburg F, Ten Harkel ADJ, Snoep MC, et al. Prenatal detection of aortic coarctation in a well-organized screening setting: Are we there yet?[J]. Prenat Diagn, 2023, 43(5): 620-628.
|
| 16 |
Geggel RL. Coarctation of the aorta: delay in diagnosis and referral basis from infancy to adulthood[J]. J Pediatr, 2022, 242: 57-62.
|
| 17 |
DeVore GR, Haxel C, Satou G, et al. Improved detection of coarctation of the aorta using speckle-tracking analysis of fetal heart on last examination prior to delivery[J]. Ultrasound Obstet Gynecol, 2021,57(2): 282-291.
|
| 18 |
Sandhu K, Pepe S, Smolich JJ, et al. Arterial stiffness in congenital heart disease[J]. Heart Lung Circ, 2021, 30(11): 1602-1612.
|
| 19 |
McFarland CA, Truong DT, Pinto NM, et al. Implications of left ventricular dysfunction at presentation for infants with coarctation of the aorta[J]. Pediatr Cardiol, 2021, 42(1): 72-77.
|
| 20 |
DeVore GR, Jone PN, Satou G, et al. Aortic coarctation: a comprehensive analysis of shape, size, and contractility of the fetal heart[J]. Fetal Diagn Ther, 2020, 47(5): 429-439.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}