
2024 , Vol. 21 >Issue 11: 1048 - 1056
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2024.11.007
多模态超声联合血清学肿瘤标志物在肺周围型病变良恶性鉴别中的应用价值
Copy editor: 吴春凤
收稿日期: 2024-04-06
网络出版日期: 2025-01-24
基金资助
国家青年岐黄学者支持项目;国家自然科学基金青年基金(81704060)安徽中医药大学2020年度科学研究项目(2020yfyzc49)
版权
Value of multimodal ultrasound combined with serum tumor markers in differential diagnosis of benign and malignant peripheral pulmonary lesions
Received date: 2024-04-06
Online published: 2025-01-24
Copyright
目的
探讨由灰阶超声、彩色多普勒超声、超声造影构成的多模态超声联合血清学肿瘤标志物组合在肺周围型病变良恶性鉴别诊断中的应用价值。
方法
回顾性分析2022年1月至2023年12月于安徽中医药大学第一附属医院行肺周围型病变超声造影检查的65例患者。按照病理结果分为良性组及恶性组,所有患者均行多模态超声检查及血清学肿瘤标志物组合检测,对获取的病灶最大径线、病灶形态、血流形态、血流信号分级、内部回声、边界、支气管征、坏死、造影剂到达病灶的始增时间(AT)、造影剂到达病灶与周围肺组织的始增时间差(TAT)、造影剂增强模式、造影剂灌注模式以及患者的血清学肿瘤标志物检测结果进行单因素分析,将单因素分析中差异有统计学意义的各因素纳入Logistic回归分析,建立肺周围型病变的多因素联合预测模型,并绘制受试者操作特征(ROC)曲线检验其诊断肺周围型病变良恶性的效能。
结果
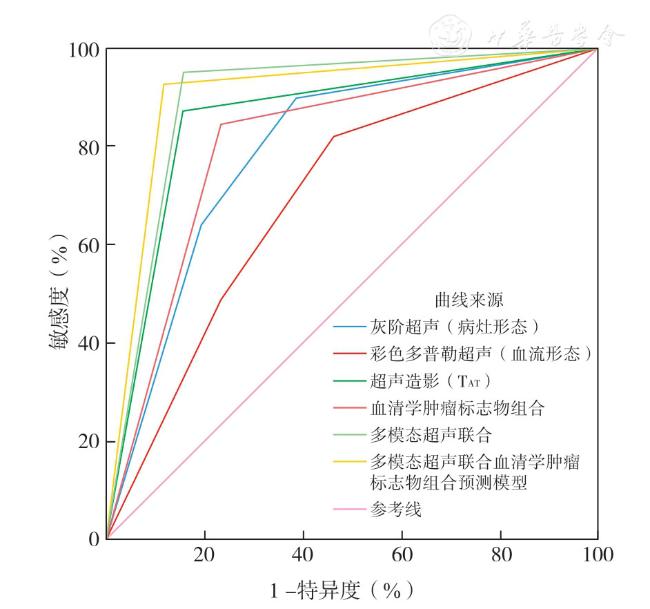
单因素结果显示灰阶超声(病灶形态)、彩色多普勒超声(血流形态)、超声造影(AT、TAT)以及血清学肿瘤标志物组合在肺周围型病变的良恶性鉴别方面具有统计学意义(P<0.05)。Logistic回归分析显示灰阶超声(病灶形态)、彩色多普勒超声(血流形态)、超声造影(TAT)、血清学肿瘤标志物组合与肺周围型病变的良恶性显著相关,回归方程式为:Logit(P)=-6.996+0.909X病灶形态+1.521X血流形态+2.927XTAT+2.553X血清学肿瘤标志物组合。绘制灰阶超声(病灶形态)、彩色多普勒超声(血流形态)、超声造影(TAT)、血清学肿瘤标志物组合、多模态超声联合以及多模态超声联合血清学肿瘤标志物预测模型的ROC曲线,其中多模态超声联合血清学肿瘤标志物预测模型曲线下面积最大(0.904)。
结论
灰阶超声(病灶形态)、彩色多普勒超声(血流形态)、超声造影(TAT)以及血清学肿瘤标志物组合在鉴别肺周围型病变良恶性方面均具有一定的诊断价值,但多模态超声联合血清学肿瘤标志物的诊断效能更高。
王瑞 , 陈炜 , 王金萍 , 李保启 . 多模态超声联合血清学肿瘤标志物在肺周围型病变良恶性鉴别中的应用价值[J]. 中华医学超声杂志(电子版), 2024 , 21(11) : 1048 -1056 . DOI: 10.3877/cma.j.issn.1672-6448.2024.11.007
Objective
To evaluate the value of multimodal ultrasound consisting of grayscale ultrasound, color Doppler flow imaging, and contrast-enhanced ultrasound (CEUS) combined with serological tumor markers in the differential diagnosis of benign and malignant peripheral pulmonary lesions.
Methods
A retrospective analysis was performed on 65 patients who underwent contrast-enhanced ultrasound examination for peripheral pulmonary lesions at the First Affiliated Hospital, Anhui University of Chinese Medicine from January 2022 to December 2023. They were divided into either a benign group or a malignant group according to the pathological results. All patients underwent multimodal ultrasound examination and detection of serological tumor markers. Lesion maximum diameter, lesion morphology, blood flow morphology, blood flow signal grade, internal echo, boundary, bronchial sign,necrosis, contrast agent arrival time (AT), the difference of arrival time between the lesion and the surrounding lung tissue (TAT), contrast agent enhancement mode, perfusion mode, and the combination of serum tumor markers were recorded for univariate analysis. All factors considered statistically significant in the univariate analysis were included in Logistic regression analysis. A multi-factor combined prediction model for peripheral pulmonary lesions was established and receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic efficiency of the model.
Results
Univariate analysis showed that there were statistically significant differences in lesion morphology on gray-scale ultrasound, blood flow morphology on Doppler flow imaging, AT and TAT on contrast-enhanced ultrasound, and the combination of serum tumor markers between benign and malignant peripheral pulmonary lesions (P<0.05). Logistic regression analysis showed that lesion morphology on gray-scale ultrasound, blood flow morphology on color Doppler flow imaging, TAT on contrast-enhanced ultrasound, and the combination of serum tumor markers were statistically significant in the differentiation of benign and malignant peripheral pulmonary lesions. The regression equation is: Logit(P)=-6.996+0.909Xlesionmorphology+1.521Xbloodflowmorphology+2.927XTAT+2.553Xthecombinationofserumtumormarkers. The ROC curves of lesion morphology on gray-scale ultrasound,blood flow morphology on color Doppler flow imaging, TAT on contrast-enhanced ultrasound, the combination of serum tumor markers, multimodal ultrasound, and multimodal ultrasound combined with serological tumor markers for the prediction of the nature of peripheral pulmonary lesions were plotted. The area under the curve of multimodal ultrasound combined with serological tumor markers was the largest (0.904).
Conclusion
Lesion morphology on gray scale ultrasound, blood flow morphology on color Doppler flow imaging, TAT on contrast-enhanced ultrasound, and the combination of serum tumor markers each have appreciated diagnostic value in differentiating benign and malignant peripulmonary lesions, but their combination has higher diagnostic efficacy.
表1 2组肺周围型病变患者基线资料比较 |
| 组别 | 例数 | 性别(例) | 年龄(岁,±s) | 吸烟史(例) | ||
|---|---|---|---|---|---|---|
| 男 | 女 | 有 | 无 | |||
| 恶性组 | 39 | 27 | 12 | 68.15±9.48 | 19 | 20 |
| 良性组 | 26 | 17 | 9 | 63.23±12.21 | 14 | 12 |
| 统计值 | χ 2=0.106 | t=1.826 | χ 2=0.164 | |||
| P值 | 0.745 | 0.073 | 0.685 | |||
表2 2组肺周围型病变患者超声特征组间比较(例) |
| 组别 | 例数 | 最大径线(mm,±s) | 病灶形态 | 血流形态 | 血流信号分级 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 楔形 | 类圆形 | 不规则形 | 无血流 | 树枝状 | 点线状 | 0~1级 | 2~3级 | ||||
| 恶性组 | 39 | 65.72±26.57 | 4 | 10 | 25 | 13 | 7 | 19 | 26 | 13 | |
| 良性组 | 26 | 59.46±24.88 | 16 | 5 | 5 | 6 | 14 | 6 | 16 | 10 | |
| 统计值 | t=0.954 | χ 2=20.417 | χ 2=9.450 | χ 2=0.179 | |||||||
| P值 | 0.344 | <0.001 | 0.009 | 0.672 | |||||||
| 组别 | 例数 | 内部回声 | 支气管征 | 边界 | 坏死 | 血清学肿瘤标志物组合 | |||||
| 均匀 | 不均匀 | 无 | 有 | 清晰 | 不清晰 | 无 | 有 | 阳性 | 阴性 | ||
| 恶性组 | 39 | 5 | 34 | 35 | 4 | 29 | 10 | 22 | 17 | 33 | 6 |
| 良性组 | 26 | 5 | 21 | 19 | 7 | 20 | 6 | 19 | 7 | 6 | 20 |
| χ 2值 | 0.492 | 3.082 | 0.055 | 1.861 | 24.615 | ||||||
| P值 | 0.483 | 0.079 | 0.814 | 0.173 | <0.001 | ||||||
| 组别 | 例数 | AT | TAT | 增强模式 | 灌注模式 | ||||||
| <10 s | ≥10 s | <2.5 s | ≥2.5 s | 均匀 | 不均 | 非向心型 | 向心型 | ||||
| 恶性组 | 39 | 1 | 38 | 5 | 34 | 11 | 28 | 12 | 27 | ||
| 良性组 | 26 | 11 | 15 | 22 | 4 | 8 | 18 | 10 | 16 | ||
| χ 2值 | 16.369 | 33.112 | 0.050 | 0.412 | |||||||
| P值 | <0.001 | <0.001 | 0.824 | 0.521 | |||||||
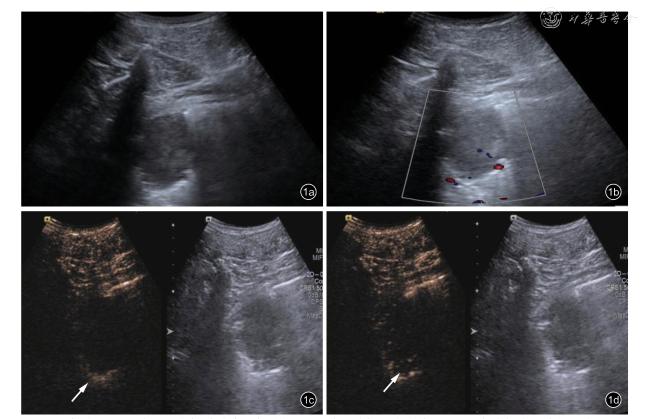
图1 男性患者,67岁,浸润性肺腺癌(低分化),右肺下叶低回声团块。图a:灰阶超声示病灶呈类圆形,边界清晰,未见支气管征,未见明显坏死;图b:彩色多普勒超声示病灶内部血流形态呈点线状,血流信号分级1级;图c:超声造影示造影剂注入11 s后,周围肺组织见造影剂进入(箭头所示);图d:超声造影示造影剂注入15 s后,病灶内可见造影剂进入(箭头所示) |
表3 肺周围型病变良恶性的多因素Logistic回归分析结果 |
| 因素 | B值 | SE值 | P值 | OR值 | OR值的95%CI |
|---|---|---|---|---|---|
| 病灶形态 | 0.909 | 0.425 | 0.033 | 2.481 | 1.079~5.709 |
| 血流形态 | 1.521 | 0.764 | 0.047 | 4.579 | 1.024~20.483 |
| AT | 2.035 | 1.387 | 0.142 | 7.651 | 0.505~65.955 |
| TAT | 2.927 | 1.110 | 0.008 | 8.667 | 2.122~74.241 |
| 血清学肿瘤标志物组合 | 2.553 | 1.193 | 0.032 | 7.841 | 1.238~69.193 |
| 常量 | -6.996 | 2.087 | 0.001 | 0.001 |
| 1 |
王慧春, 王玉斌, 崔兰兰, 等. 肺癌18F-FDG PET/CT代谢特征与肿瘤标志物的相关性[J]. 中国医学影像学杂志, 2020, 28(5): 343-348.
|
| 2 |
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries [J]. CA Cancer J Clin, 2018, 68(6): 394-424.
|
| 3 |
Zhang HX, Guang Y, He W, et al. Ultrasound-guided percutaneous needle biopsy skill for peripheral lung lesions and complications prevention [J]. J Thorac Dis, 2020, 12(7): 3697-3705.
|
| 4 |
Bi K, Zhou RR, Zhang Y, et al. US contrast agent arrival time difference ratio for benign versus malignant subpleural pulmonary lesions [J]. Radiology, 2021, 301(1): 200-210.
|
| 5 |
Bi K, Xia DM, Fan L, et al. Development and prospective validation of an ultrasound prediction model for the differential diagnosis of benign and malignant subpleural pulmonary lesions: a large ambispective cohort study [J]. Front Oncol, 2021, 11: 656060.
|
| 6 |
Piscaglia F, Nolsøe C, Dietrich C, et al. The EFSUMB guidelines and recommendations on the clinical practice of contrast enhanced ultrasound (CEUS): update 2011 on non-hepatic applications [J].Ultraschall in Der Medizin, 2011, 33(1): 33-59.
|
| 7 |
Bai J, Yang W , Wang S, et al. Role of arrival time difference between lesions and lung tissue on contrast-enhanced sonography in the differential diagnosis of subpleural pulmonary lesions [J]. J Ultrasound Med, 2016, 35(7): 1523-1532.
|
| 8 |
陈霰, 徐丽伟, 邢恩芳, 等. 超声造影及介入在周围型肺部病变诊断中的价值 [J]. 中国超声医学杂志, 2015, 31(12): 1080-1082.
|
| 9 |
查俪晶, 闻卿, 徐雯, 等. 超声造影在局灶性机化性肺炎与原发性肺癌鉴别诊断中的价值 [J]. 中华超声影像学杂志, 2018, 27(8):688-691.
|
| 10 |
杨继辉, 朱灿, 沈严严, 等. 三阴性乳腺癌超声征象与P53的相关性 [J]. 中国医学影像学杂志, 2019, 27(2): 97-101.
|
| 11 |
韩红, 丁红, 季正标, 等. 微血流成像技术在肝肿瘤血流检测中的应用价值及与彩超的比较研究 [J]. 中国超声医学杂志, 2019, 35(4):331-334.
|
| 12 |
姜明, 臧爱华, 季旸, 等. 超声造影联合肺癌血清检测指标对周围型肺病变的诊断效能[J]. 中国超声医学杂志, 2021, 37(5): 520-522.
|
| 13 |
张怡, 毕珂, 朱惠铭, 等. 超声造影定量分析在胸膜下肺病灶良恶性鉴别中的诊断价值 [J]. 中华航海医学与高气压医学杂志, 2021,28(4): 494-498.
|
| 14 |
李琪, 聂芳, 杨丹, 等. 超声造影定量分析联合肿瘤标记物在肺周围型病灶良恶性诊断中的价值 [J]. 中华超声影像学杂志, 2017,26(8): 682-686.
|
| 15 |
Wei H, Lu Y, Ji Q, et al. The application of conventional us and transthoracic ultrasound elastography in evaluating peripheral pulmonary lesions [J]. Exp Ther Med, 2018, 16(2): 1203-1208.
|
| 16 |
郑小雪, 唐敏, 魏国李, 等. 常规超声、超声造影及肿瘤标志物联合评分在肺周围型病变良恶性诊断中的价值 [J]. 临床超声医学杂志, 2020, 22(3): 184-188.
|
| 17 |
李敏, 李海文, 陶运亮, 等. 超声造影定量参数对肺部良恶性病变鉴别诊断的价值研究[J]. 重庆医学, 2020, 49(16): 2686-2689, 2693.
|
| 18 |
陈松丽, 吴正华, 张诚. 实时超声造影在胸膜下肺肿块中的应用价值 [J]. 中国超声医学杂志, 2022, 38(1): 26-29.
|
| 19 |
Li Q, Nie F, Yang D, et al. Role of contrast-enhanced ultrasound in pulmonary lesions: 5-year experience at a single center [J]. Ultrasound Med Biol, 2021, 48(2): 257-264.
|
| 20 |
Wei H, Wang Y, Li J, et al. Diagnosis of benign and malignant peripheral lung lesions based on a feature model constructed by the random forest algorithm for grayscale and contrast-enhanced ultrasound [J]. Front Oncol, 2024, 14: 1352028.
|
| 21 |
杨瑞静, 杨一林, 阮骊韬, 等. 超声在肺周围型病变良恶性判定中的诊断价值 [J]. 临床超声医学杂志, 2012, 14(7): 454-456.
|
| 22 |
Gorg C. Transcutaneous contrast-enhanced sonography of pleural based pulmonary lesions [J]. Eur J Radiol, 2007, 64(2): 213-221.
|
| 23 |
Bai Z, Liu T, Liu W, et al. Application value of contrast-enhanced ultrasound in the diagnosis of peripheral pulmonary focal lesions [J].Medicine, 2022, 101(29): e29605.
|
| 24 |
唐敏, 宋建琼, 郑小雪, 等. 病灶-肺组织造影剂到达时间差对富血供肺周围型病变的诊断价值 [J]. 中国超声医学杂志, 2019,35(10): 894-897.
|
| 25 |
Tang M, Xie Q, Wang J, et al. Time difference of arrival on contrastenhanced ultrasound in distinguishing benign inflammation from malignant peripheral pulmonary lesions [J]. Front Oncol, 2020, 10:578884.
|
| 26 |
李倩倩, 薛洁, 姜静. 超声造影结合肿瘤标记物对肺周围型占位性病变性质的诊断效果研究 [J]. 湖南师范大学学报(医学版), 2020,17(1): 165-168.
|
| 27 |
吴霞玲, 孟娜, 黄星月, 等. 超声造影时间-强度曲线在肺周围性病变及胸腺肿瘤诊断中的应用价值 [J]. 武汉大学学报(医学版),2015, 36(3): 6.
|
| 28 |
Shen M, Bi K, Cong Y, et al. Application of contrast-enhanced ultrasound in the differential diagnosis of benign and malignant subpleural pulmonary lesions [J]. J Ultrasound Med, 2022, 41(5):1147-1157.
|
| 29 |
王凇. 新型超声造影微血管灌注模式对周围型肺占位的鉴别诊断[J]. 中华超声影像学杂志, 2014, 23(5): 408-413.
|
| 30 |
唐敏, 宋建琼, 郑小雪, 等. 富血供肺周围型病变的超声造影实时分析 [J]. 中国超声医学杂志, 2019, 35(9): 776-779.
|
| 31 |
梁汝娜, 王娟, 张伟, 等. 超声造影与高分辨率CT鉴别诊断周围型肺肿物的价值 [J].中国CT和MRI杂志, 2023, 21(3): 68-70.
|
| 32 |
陈倩倩, 宋佳, 孙淑艳. 五种肿瘤标志物联合检测在肺癌诊断中的价值 [J]. 中国老年学杂志, 2018, 38(7): 1597-1598.
|
| 33 |
张婷, 向波, 林勇平. 肿瘤标志物联合检测在肺癌辅助诊断中的预测价值 [J]. 中华预防医学杂志, 2021, 55(6): 786-791.
|
| 34 |
陈俊峰. 彩色多普勒超声及肿瘤标志物联合诊断肺周围型占位病变的价值分析 [J]. 中国医疗器械信息, 2023, 29(10): 10-12, 23.
|
| 35 |
万里, 赵岭. 病变-肺组织始增时间差联合血清肿瘤标记物对肺周围型病变的诊断价值 [J]. 中华超声影像学杂志, 2021, 30(11): 950-954.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}