
2025 , Vol. 22 >Issue 01: 15 - 24
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.01.003
富血供子宫肌瘤超声造影特征及其组织病理学相关性
Copy editor: 吴春凤
收稿日期: 2024-09-03
网络出版日期: 2025-04-18
基金资助
国家自然科学基金(82272004,81974470)浙江省自然科学基金(LZ22H180001)
版权
Contrast-enhanced ultrasound features of highly vascularized uterine leiomyoma and their correlation with pathology
Received date: 2024-09-03
Online published: 2025-04-18
Copyright
目的
探讨不同病理类型富血供子宫肌瘤超声造影特征及其与组织病理学的相关性,为临床治疗方案的选择提供影像学依据。
方法
收集2021 年6 月至2023 年10 月在浙江大学医学院附属妇产科医院因子宫肌瘤住院并进行手术治疗的病例78 例,共计97 枚病灶,均经彩色/能量多普勒超声检查诊断为富血供的子宫肌瘤,术前均行超声造影检查。根据组织病理学结果将病灶分为普通子宫肌瘤组、普通子宫肌瘤变性组、特殊类型子宫肌瘤组及子宫肉瘤组4 组进行比较;再将普通子宫肌瘤变性组中水肿变性子宫肌瘤、透明变性子宫肌瘤和特殊类型子宫肌瘤组中富细胞性平滑肌瘤与普通子宫肌瘤组进行比较。使用Fisher 确切概率法比较组间超声造影特征整体差异,采用Bonferroni 检验进行两两比较,分析比较各组病灶造影剂到达时间、达峰时间及增强晚期病灶内造影剂消退快慢及强化程度的超声造影模式之间的差异。
结果
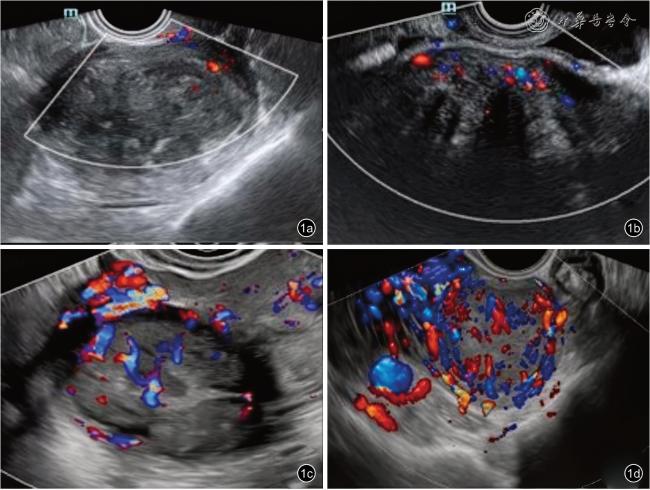
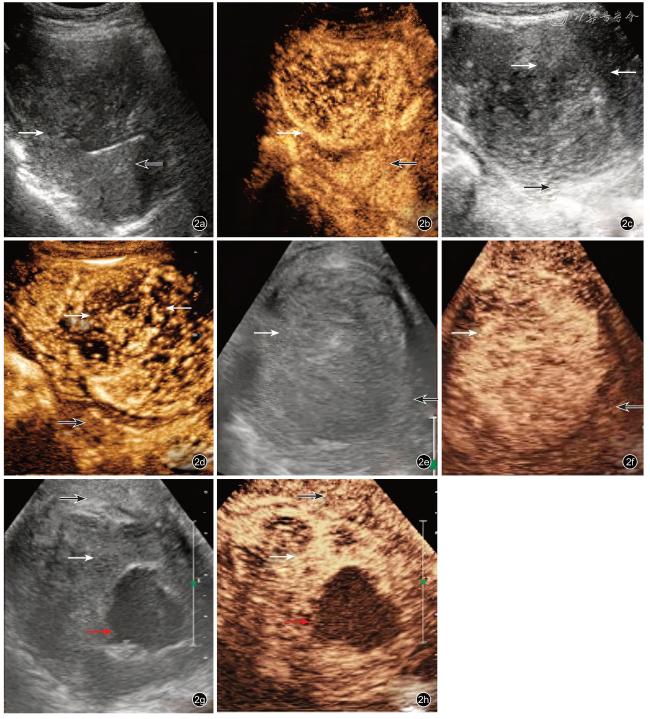
97 枚彩色/能量多普勒超声检查诊断为富血供子宫肌瘤中93 枚(95.9%)最终经组织病理学诊断为良性子宫肌瘤,4 枚(4.1%)诊断为恶性子宫肉瘤。普通子宫肌瘤组(51 枚)、普通子宫肌瘤变性组(23 枚)、特殊类型子宫肌瘤组(19 枚)与子宫肉瘤组(4 枚)4 组比较造影剂到达时间(P=0.004),达峰时病灶强化程度(P=0.013)、内部造影剂分布均匀性(P<0.001),增强晚期病灶内造影剂消退快慢(P<0.001)、病灶强化程度(P=0.005)差异均具有统计学意义;普通子宫肌瘤组(51 枚)与普通子宫肌瘤水肿变性组(11 枚)、普通子宫肌瘤透明变性组(10 枚)和富细胞性平滑肌瘤组(11 枚)4 组比较:造影剂到达时间(P=0.001),达峰时病灶强化程度(P=0.014)、内部造影剂分布均匀性(P<0.001),增强晚期病灶内造影剂消退快慢(P<0.001)差异均具有统计学意义,增强晚期病灶强化程度差异无统计学意义(P=0.329)。不同病理类型富血供子宫肌瘤超声造影增强模式表现为:(1)普通子宫肌瘤组以同步均匀性等增强模式为主;(2)普通子宫肌瘤变性组达峰时不均匀性增强比例较高,其中水肿变性以快进高增强模式为主,内见“筛孔状”低灌注区;透明变性以同步等增强或低增强模式为主;(3)子宫肉瘤组快进快出不均匀性高增强比例最高,其中3 枚(75.0%)病灶可见“地图样”不规则无灌注区域;(4)特殊类型子宫肌瘤组中富细胞性平滑肌瘤快进高增强比例较高,但低于子宫肉瘤组,达峰时病灶内部造影剂分布较均匀。
结论
不同病理类型的富血供子宫肌瘤超声造影模式之间存在差异,这些差异特征有助于术前推断其组织病理学类型,为临床决策提供影像学依据。
于爽 , 王茜 , 方昀 , 陈敏 , 王立臣 , 朱江 . 富血供子宫肌瘤超声造影特征及其组织病理学相关性[J]. 中华医学超声杂志(电子版), 2025 , 22(01) : 15 -24 . DOI: 10.3877/cma.j.issn.1672-6448.2025.01.003
Objective
To explore the correlation between contrast-enhanced ultrasound (CEUS)characteristics and pathology of highly vascularized uterine leiomyoma, in order to provide a reliable imaging basis for the selection of clinical treatment.
Methods
A total of 78 patients who were hospitalized and underwent surgical treatment for uterine leiomyoma in the Women’s Hospital School of Medicine Zhejiang University from June 2021 to October 2023 were collected.Finally, 97 lesions were diagnosed as highly vascularized uterine leiomyoma by color/energy Doppler ultrasonography, all of which underwent contrastenhanced ultrasound before surgery.According to pathology, the 97 lesions were divided into common uterine leiomyomas, common uterine leiomyomas with degeneration, special types of uterine leiomyomas,and uterine sarcoma for comparison.The edematous uterine leiomyomas and uterine leiomyomas with hyaline degeneration in the common leiomyomas with degeneration group, and the cellular leiomyomas in the special leiomyoma group were also compared with the common uterine leiomyomas group.Fisher exact probability method was used to compare the overall difference between groups, and Bonferroni test was used for pairwise comparisons.The contrast-enhanced ultrasound mode features, arrival time, time to peak,and late enhancement features were also compared among the groups.
Results
Ninety-three (95.9%) of 97 highly vascularized uterine leiomyomas diagnosed by color/energy Doppler ultrasonography were eventually diagnosed as benign leiomyoma by histopathology, and four (4.1%) were diagnosed as uterine sarcomas.The arrival time (P=0.004), the degree of enhancement at the peak (P=0.013), the uniformity of internal contrast distribution (P<0.001), the speed of wash-out (P<0.001), and the degree of lesion enhancement (P=0.005)differed significantly among the common uterine leiomyomas group (51 lesions), the uterine leiomyomas with degeneration group (23 lesions), the special type of uterine leiomyomas group (19 lesions), and the uterine sarcomas group (4 lesions).There were significant differences in the arrival time (P=0.001), the degree of enhancement (P=0.014), the uniformity of internal contrast distribution (P<0.001), and the speed of washout (P<0.001) among common leiomyoma (51 lesions), edematous uterine leiomyomas (11 lesions) and uterine leiomyomas with hyaline degeneration (11 lesions) in the common leiomyomas with degeneration group, and cellular leiomyomas (11 lesions) in the special type of leiomyomas group, though there was no significant difference in the degree of enhancement in the late stage of enhancement (P=0.329).The contrastenhanced ultrasound patterns of different pathology classifications of highly vascularized uterine leiomyoma were as follows: (1) The enhanced mode such as synchronous uniformity and equal enhanced ratio was higher in the common leiomyomas group; (2) The time to peak and inhomogeneity enhancement ratio was higher in the common leiomyomas with degeneration group.The fast-in hyperenhancement pattern was the main pattern of edematous degeneration, “honeycomb-like” hypoperfusion areas were seen internally,and hyaline degeneration was dominated by synchronous equal enhancement or low enhancement patterns;(3) The uterine sarcomas group had the highest proportion fast wash-out and inhomogeneity enhancement,and 3 lesions (75.0%) showed non-perfusion areas of “map pattern”; and (4) The proportion of cellular leiomyomas in the special type of leiomyomas group with fast-in and high enhancement was high, but lower than that of the uterine sarcoma group.
Conclusion
There are differences in contrast-enhanced ultrasound patterns between different pathologic types of highly vascularized uterine leiomyomas and uterine sarcomas.These differences can help to infer the pathology classification before surgery and provide an imaging basis for clinical decision-making.
Key words: Uterine leiomyoma; Ultrasound; Contrast-enhanced ultrasound; Pathology
 ±s 表示,CEUS 检查时间与手术时间间隔为服从偏态分布的计量资料,采用M(QR)表示;患者临床症状、病理结果及CEUS 特征为计数资料,使用例数与构成比描述,使用Fisher 确切概率法比较组间整体差异性,再利用Bonferroni 方法进行组间多重比较。P<0.05 表示差异有统计学意义。
±s 表示,CEUS 检查时间与手术时间间隔为服从偏态分布的计量资料,采用M(QR)表示;患者临床症状、病理结果及CEUS 特征为计数资料,使用例数与构成比描述,使用Fisher 确切概率法比较组间整体差异性,再利用Bonferroni 方法进行组间多重比较。P<0.05 表示差异有统计学意义。表1 不同病理类型子宫肌瘤患者超声造影特征比较[枚(%)] |
| 项目 | 普通子宫肌瘤组(n=51) | 普通子宫肌瘤变性组(n=23) | 特殊类型子宫肌瘤组(n=19) | 子宫肉瘤组(n=4) | P 值 |
|---|---|---|---|---|---|
| 增强早期 | |||||
| 造影剂到达时间 | 0.004 | ||||
| 早 | 9(17.6) | 8(34.8) | 8(42.1) | 4(100)a | |
| 同步 | 34(66.7) | 11(47.8) | 5(26.3)a | 0(0)a | |
| 晚 | 8(15.7) | 4(17.4) | 6(31.6) | 0(0) | |
| 达峰时 | |||||
| 强化程度 | 0.013 | ||||
| 高增强 | 10(19.6) | 8(34.8) | 7(36.8) | 4(100)a | |
| 等增强 | 29(56.9) | 12(52.2) | 5(26.3) | 0(0) | |
| 低增强 | 12(23.5) | 3(13.0) | 7(36.8) | 0(0) | |
| 分布 | < 0.001 | ||||
| 均匀 | 49(96.1) | 7(30.4) | 14(73.7)ab | 1(25.0)a | |
| 不均匀 | 2(3.9) | 16(69.6) | 5(26.3)ab | 3(75.0)a | |
| 增强晚期 | |||||
| 造影剂消退 | < 0.001 | ||||
| 早 | 3(5.9) | 2(8.7) | 4(21.1) | 4(100)abc | |
| 同步 | 43(84.3) | 14(60.9) | 7(36.8)a | 0(0)a | |
| 晚 | 5(9.8) | 7(30.4) | 8(42.1)a | 0(0) | |
| 强化程度 | 0.005 | ||||
| 高增强 | 9(17.6) | 0(0) | 5(26.3) | 3(75.0)ab | |
| 等增强 | 27(52.9) | 17(73.9) | 7(36.8) | 0(0)b | |
| 低增强 | 15(29.4) | 6(26.1) | 7(36.8) | 1(25.0) |
注:a 与普通子宫肌瘤组比较,b 与普通子宫肌瘤变性组比较,c 与特殊类型子宫肌瘤组比较,差异具有统计学意义(P<0.05) |
表2 不同病理类型亚型子宫肌瘤患者超声造影特征比较[枚(%)] |
| 项目 | 普通子宫肌瘤组(n=51) | 普通子宫肌瘤水肿变性组(n=11) | 普通子宫肌瘤透明变性组(n=10) | 富细胞性平滑肌瘤组(n=11) | P 值 |
|---|---|---|---|---|---|
| 增强早期 | |||||
| 造影剂到达时间 | 0.001 | ||||
| 早 | 9(17.6) | 7(63.6)a | 1(10.0) | 8(72.7)ab | |
| 同步 | 34(66.7) | 3(27.3) | 6(60.0) | 2(18.2)a | |
| 晚 | 8(15.7) | 1(9.1) | 3(30.0) | 1(9.1) | |
| 达峰时 | 0.014 | ||||
| 强化程度 | |||||
| 高增强 | 10(19.6) | 6(54.5) | 1(10.0) | 7(63.6)a | |
| 等增强 | 29(56.9) | 4(36.4) | 5(50.0) | 4(36.4) | |
| 低增强 | 12(23.5) | 1(9.1) | 4(40.0) | 0(0) | |
| 分布 | < 0.001 | ||||
| 均匀 | 49(96.1) | 5(45.5)a | 2(20.0)a | 9(81.8)b | |
| 不均匀 | 2(3.9) | 6(54.5)a | 8(80.0)a | 2(18.2)b | |
| 增强晚期 | |||||
| 造影剂消退 | < 0.001 | ||||
| 早 | 3(5.9) | 2(18.2) | 0(0) | 7(63.6)ab | |
| 同步 | 43(84.3) | 5(45.5)a | 5(50.0) | 3(27.3)a | |
| 晚 | 5(9.8) | 4(36.4) | 5(50.0)a | 1(9.1) | |
| 强化程度 | 0.329 | ||||
| 高增强 | 9(17.6) | 0(0) | 0(0) | 3(27.3) | |
| 等增强 | 27(52.9) | 8(72.7) | 5(50.0) | 4(36.4) | |
| 低增强 | 15(29.4) | 3(27.3) | 5(50.0) | 4(36.4) |
注:a 与普通子宫肌瘤组比较,b 与普通子宫肌瘤透明变性组比较,差异具有统计学意义(P<0.05) |
| 1 |
Yang Q, Ciebiera M, Bariani M, et al.Comprehensive review of uterine fibroids: developmental origin, pathogenesis, and treatment [J].Endocr Rev, 2022, 43(4): 678-719.
|
| 2 |
Vu K, Fast A, Shaffer R, et al.Evaluation of the routine use of pelvic MRI in women presenting with symptomatic uterine fibroids: when is pelvic MRI useful? [J].J Magn Reson Imaging, 2019, 49(7): 271-281.
|
| 3 |
Awiwi MO, Badawy M, Shaaban AM, et al.Review of uterine fibroids:imaging of typical and atypical features, variants, and mimics with emphasis on workup and FIGO classification [J].Abdom Radiol(NY),2022, 47(7): 2468-2485.
|
| 4 |
Devereaux KA, Schoolmeester JK.Smooth muscle tumors of the female genital tract [J].Surg Pathol Clin, 2019, 12(2): 397-455.
|
| 5 |
Robboy SJ, Bentley RC, Butnor K, et al.Pathology and pathophysiology of uterine smooth-muscle tumors [J].Environ Health Perspect, 2000, 108(Supple5): 779-784.
|
| 6 |
WHO Classification of Tumours Editorial Board [M].Lyon(France):IARC Publications, 2020: 1-632.
|
| 7 |
Putra AD, Maharani N, Gianina K.Ultrasound features and diagnostic workup of uterine leiomyosarcomas [J].J Ultrasound Med, 2021,41(7): 1837-1844.
|
| 8 |
Sabrina C, Mojgan D, Patricia P, et al.Uterine sarcomas and rare uterine mesenchymal tumors with malignant potential.Diagnostic guidelines of the French Sarcoma Group and the Rare Gynecological Tumors Group [J].Gynecol Oncol, 2022, 167(2): 373-389.
|
| 9 |
Di Giuseppe J, Grelloni C, Giuliani L, et al.Recurrence of uterine smooth muscle tumor of uncertain malignant potential: a systematic review of the literature [J].Cancers, 2022, 14(9): 2323-2337.
|
| 10 |
Gitas G, Ertan K, Baum S, et al.Effect of tumor morcellation in patients with early uterine sarcoma: a multicenter study in Germany [J].J Turk Ger Gynecol Assoc, 2022, 23(2): 75-82.
|
| 11 |
Mathew RP, Francis S, Jayaram V, et al.Uterine leiomyomas revisited with review of literature [J].Abdom Radiol (NY), 2021, 46(10): 4908-4926.
|
| 12 |
Russo C, Camilli S, Martire F, et al.Ultrasound features of highly vascularized uterine myomas (uterine smooth muscle tumors) and correlation with histopathology [J].Ultrasound Obstet Gynecol, 2022,60(2): 269-267.
|
| 13 |
Ludovisi M, Moro F, Pasciuto T, et al.Imaging in gynecological disease (15): clinical and ultrasound characteristics of uterine sarcoma[J].Ultrasound Obstet Gynecol, 2019, 54(5): 676-687.
|
| 14 |
Luo W, Zhang P, Yang X, et al.Role of contrast-enhanced ultrasonography in MR-guided focused ultrasound ablation on uterus fibroids: lesion selection and assessment of ablative effects [J].Eur Radiol, 2021, 32(3): 2110-2119.
|
| 15 |
Van den Bosch T, Dueholm M, Leone FPG, et al.Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group [J].Ultrasound Obstet Gynecol, 2015, 46(3): 284-298.
|
| 16 |
中国医师协会超声医师分会.妇产科疾病静脉超声造影临床应用中国专家共识(2023 版) [J].中华超声影像学杂志, 2023, 32(7):553-564.
|
| 17 |
温博, 张晶, 冯蕾, 等.磁共振成像对超声引导经皮微波消融治疗子宫肌瘤近期效果的预测研究 [J/CD].中华医学超声杂志(电子版), 2015, 12(7): 574-578.
|
| 18 |
Ahmad A, Kumar M, Bhoi N.Diagnosis and management of uterine fibroids: current trends and future strategies [J].J Basic Clin Physiol Pharmacol, 2023, 34(3): 291-310.
|
| 19 |
Pysz MA, Willmann JK.Targeted contrast-enhanced ultrasound:an emerging technology in abdominal and pelvic imaging [J].Gastroenterology, 2011, 140(3): 785-790.
|
| 20 |
杨晓, 罗文, 张佩蒂, 等.超声造影在磁共振引导聚焦超声治疗子宫肌瘤患者术前筛选中的作用 [J].中华超声影像学杂志, 2021,30(7): 575-579.
|
| 21 |
Stoelinga B, Dooper A, Juffermans L, et al.Use of contrast-enhanced ultrasound in the assessment of uterine fibroids: a feasibility study [J].Ultrasound Med Biol, 2018, 44(8): 1901-1909.
|
| 22 |
Don E, Landman A, Vissers G, et al.Uterine fibroids causing preterm birth: a new pathophysiological hypothesis on the role of fibroid necrosis and inflammation [J].Int J Mol Sci, 2022, 23(15): 8064-8072.
|
| 23 |
Sotomayor CG, Parra C, Miranda M, et al.Hyaline and cystic degeneration of uterine leiomyomas: CT and MR imaging with histopathological sample analyses [J].Diagnostics, 2023, 13(20):3230-3235.
|
| 24 |
邱冬, 常才.子宫肌瘤水肿变性的彩色多普勒超声表现及其病理基础 [J].中华超声影像学杂志, 2001, 10(11): 703-704.
|
| 25 |
Agarwal C, Pujani M, Chauhan V, et al.Cellular leiomyoma versus endometrial stromal sarcoma: a report of a rare case presenting a diagnostic challenge on intraoperative frozen section [J].Gynecol Minim Invasive Ther, 2022, 11(3): 182-184.
|
| 26 |
Hodgson A, Swanson D, Tang S, et al.Gene fusions characterize a subset of uterine cellular leiomyomas [J].Genes Chromosomes Cancer, 2020, 59(12): 688-696.
|
| 27 |
Nava H.Highly cellular leiomyoma mixed with a focus of adenomyosis [J].Cureus, 2022, 4(8): 8129-8132.
|
| 28 |
郑妩妩, 朱剑, 鲁爱慧, 等.肿瘤体积倍增时间在鉴别子宫肉瘤与富于细胞型平滑肌瘤中的作用 [J/OL].中华医学超声杂志(电子版), 2023, 20(1): 35-40.
|
| 29 |
Huang TT, Chen CM, Lin SS, et al.E7050 suppresses the growth of multidrug-resistant human uterine sarcoma by inhibiting angiogenesis via targeting of VEGFR2-mediated signaling pathways [J].Int J Mol Sci, 2023, 24(11): 9606-9617.
|
| 30 |
Libertini M, Hallin M, Thway K, et al.Gynecological sarcomas:molecular characteristics, behavior, and histology-driven therapy [J].Int J Surg Pathol, 2020, 29(1): 4-20.
|
| 31 |
Niu S, Zheng W.Endometrial stromal tumors: diagnostic updates and challenges [J].Sem Diagn Pathol, 2022, 39(3): 201-212.
|
| 32 |
Chapel DB, Maccio L, Bragantini E, et al.Dedifferentiated leiomyosarcoma of the uterus: a clinicopathologic and immunohistochemical analysis of 23 cases [J].Histopathology, 2023,82(6): 812-825.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}