
2025 , Vol. 22 >Issue 01: 31 - 38
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.01.005
281 例胎儿后颅窝池畸形的超声诊断及漏误诊分析
Copy editor: 吴春凤
收稿日期: 2024-09-27
网络出版日期: 2025-04-18
基金资助
湖北省卫生健康委员会重点项目(WJ2023Z007)
版权
Ultrasound diagnosis and causes of missed and misdiagnosis of fetal cystic malformations of the posterior fossa: analysis of 281 cases
Received date: 2024-09-27
Online published: 2025-04-18
Copyright
目的
探讨超声诊断胎儿后颅窝池畸形的准确性,进一步提升对后颅窝池畸形的认识及鉴别诊断能力。
方法
回顾性分析2020 年8 月至2023 年8 月于湖北省妇幼保健院经超声诊断为胎儿后颅窝池畸形的281 例孕妇(异常组)的病例资料,所有病例经MRI 或产后病理检查进行了确认,并与同时期2000 例正常孕妇(正常组)的年龄与孕周分布进行对比。总结胎儿后颅窝池畸形的超声诊断特征,统计超声诊断符合率,分析畸形类型分布特征及漏误诊病例的影像学特征和原因。
结果
后颅窝池畸形胎儿中超声诊断与MRI 诊断相符的病例为268 例(95.37%),超声诊断与MRI诊断不相符的病例为13 例。异常组与正常组孕妇年龄均主要集中于25~34 岁之间,分别为74.3%(199/268)和79.9%(1598/2000),差异无统计学意义(P>0.05);超声诊断胎儿后颅窝池畸形多数于孕晚期(30~34+6 周,67.5%,181/268),常可伴发神经系统畸形或其他类型的先天性异常,正常孕妇的检查孕周主要是20~22 周及30~32 周的2 次系统检查,2 组检查孕周比较差异具有统计学意义(P<0.001)。超声检出的后颅窝池畸形病种包括单纯后颅窝池增宽255 例,Dandy-Walker 畸形8例,Blake 囊肿3 例和小脑蚓部发育不良2 例。13 例误诊病例中,2 例蛛网膜囊肿误诊为Blake 囊肿,1 例蛛网膜囊肿、1 例Blake 囊肿及1 例小脑蚓部发育不良漏诊。22.8%(61/268)的病例合并其他系统畸形。后颅窝池宽度≥1.20 cm 的病例合并其他异常率为24.8%(34/137),高于宽度<1.20 cm组的13.6%(16/118)。
结论
超声检查在胎儿后颅窝池畸形的产前筛查中具有较高的诊断价值,但对于小脑蚓部发育不良及Blake 囊肿等复杂畸形还存在一定漏误诊率。孕晚期(30~34+6 周)是超声诊断后颅窝池畸形确诊的关键时期,对超声检查可疑病例建议进行全面神经系统评估及多系统联合筛查,同时进行多模态影像学验证,以提高诊断准确性。
刘福 , 王玉波 , 马以玲 , 陈诺 , 成晨 , 赵胜 . 281 例胎儿后颅窝池畸形的超声诊断及漏误诊分析[J]. 中华医学超声杂志(电子版), 2025 , 22(01) : 31 -38 . DOI: 10.3877/cma.j.issn.1672-6448.2025.01.005
Objective
To assess the diagnostic accuracy of ultrasound in detecting fetal cystic malformations of the posterior fossa in order to further enhance their diagnostic recognition and differential diagnosis.
Methods
Data of 281 fetuses (abnormal group) diagnosed with cystic malformations of the posterior fossa via ultrasound at Hubei Maternal and Child Health Hospital from August 2020 to 2023 were retrospectively analyzed.All cases were confirmed by MRI or postpartum pathological examination and compared with 2000 normal pregnant women (normal group) in the same period.The ultrasound diagnostic features of cystic malformations of the posterior fossa were summarized, the diagnostic concordance rate was calculated, the distribution of malformation types was examined, and the imaging features and causes of misdiagnosed cases were analyzed.
Results
Among all fetal posterior fossa malformation cases, ultrasound and MRI diagnoses showed concordant results in 268 cases (95.37%) and discordant results in 13.Most pregnant women in both the abnormal (74.3%, 199/268) and normal (79.9%, 1598/2000) groups were aged 25-34 years, with no significant difference between the two groups (P=0.104).Most ultrasonographic diagnoses of cystic malformations of the posterior fossa were made in late pregnancy (30-34+6 weeks, 67.5%,181/268).These malformations often coexisted with nervous system malformations or other congenital abnormalities.In contrast, normal pregnant women mainly had check-ups at 20-22 and 30-32 weeks (two systematic checks), with a significant difference in peak timing of check-ups compared to the abnormal group (P<0.001).The posterior fossa cisterna malformations detected by ultrasound included 255 cases of mega cisterna magna, 8 cases of Dandy-Walker malformation, 3 cases of Blake’s pouch cysts, and 2 cases of cerebellar vermis hypoplasia.Among 13 misdiagnosed cases, 2 arachnoid cysts were misdiagnosed as Blake's pouch cysts, and 1 case each of arachnoid cyst, Blake's pouch cyst, and cerebellar vermis hypoplasia was missed.Approximately 22.8% (61/268) of the cases had malformations in other systems.The abnormality rate was 24.8% (34/137) in the posterior cranial fossa width ≥1.20 cm group, higher than the 13.6% (16/118) in the<1.20 cm group.
Conclusion
Ultrasound is valuable for prenatal screening of cystic malformations of the posterior fossa but has a misdiagnosis rate for complex malformations like cerebellar vermis hypoplasia and Blake’s pouch cysts.Late pregnancy (30-34+6 weeks) is the critical time point for confirming these diagnoses.For suspicious cases, a comprehensive neurological assessment, multi-system screening, and multi-modality imaging verification are recommended to enhance diagnostic accuracy.
表1 2 组孕妇年龄分布比较[例(%)] |
| 组别 | 例数 | ≤ 19 岁 | 20 ~ 24 岁 | 25 ~ 29 岁 | 30 ~ 34 岁 | 35 ~ 39 岁 | 40 ~ 44 岁 |
|---|---|---|---|---|---|---|---|
| 异常组 | 268 | 2(0.2) | 20(7.5) | 100(37.3) | 99(36.9) | 40(14.9) | 7(2.6) |
| 正常组 | 2000 | 4(0.7) | 112(5.6) | 765(38.3) | 833(41.7) | 261(13.0) | 25(1.2) |
| χ 2 值 | 9.138 | ||||||
| P 值 | 0.104 |
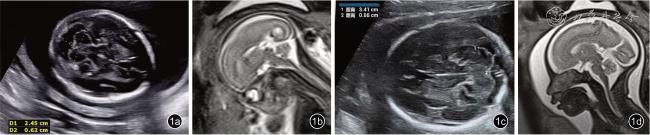
图1 正常胎儿的超声经小脑横切面与MRI 正中矢状面图像。图a 为孕23.0 周正常胎儿超声图像,图b 为孕23.0 周正常胎儿MRI 图像,图c 为孕28.1 周正常胎儿超声图像,图d 为孕28.1 周正常胎儿MRI 图像 |
表2 2 组孕妇临床孕周分布比较[例(%)] |
| 组别 | 例数 | 20 ~ 24+6周 | 25 ~ 29+6周 | 30 ~ 34+6周 | 35~ 37 周 |
|---|---|---|---|---|---|
| 异常组 | 268 | 20(7.5) | 53(19.8) | 181(67.5) | 14(5.2) |
| 正常组 | 2000 | 697(34.9) | 260(13.0) | 517(25.8) | 526(26.3) |
| χ 2 值 | 388.523 | ||||
| P 值 | < 0.001 |
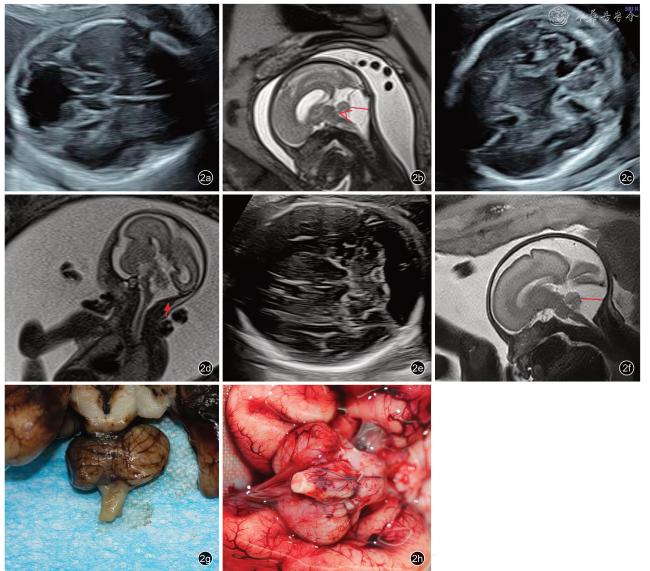
图2 后颅窝池畸形胎儿影像及病理图。图a:孕22.4 周胎儿Dandy-Walker畸形,超声经小脑横切面见后颅窝池增宽,第四脑室与后颅窝池相通,小脑蚓部显示极差;MRI 正中矢状切面(图b)见小脑蚓部上抬,角度约47°,小脑蚓部发育不良,分叶发育不完全,后颅窝池增宽。图c:孕23.6 周胎儿Blake囊肿,超声经小脑横切面可见典型的“钥匙孔征”,MRI 正中矢状切面(图d)可见菲薄的囊壁(箭头所示)。孕30.4 周单纯后颅窝池增宽胎儿超声经小脑横切面(图e)、MRI 正中矢状切面(图f)见增宽的后颅窝池,小脑、小脑蚓部形态位置正常,颅内未见其他异常。图g 为Dandy-Walker 畸形大体图,可见发育不良的小脑蚓部,蚓部下方部分缺失;图h 为小脑蚓部发育不良大体图,可见蚓部形态完整,但整体偏小 |
表3 超声诊断后颅窝池畸形病例合并其他异常情况 |
| 合并其他异常的类型 | 例数 |
|---|---|
| 合并单个系统异常 | 56 |
| 神经系统异常 | 35 |
| 侧脑室增宽 | 25 |
| 脑积水 | 3 |
| 脑膜膨出 | 2 |
| 丘脑后蛛网膜囊肿 | 1 |
| 室管膜下囊肿 | 1 |
| 胼胝体发育不良 | 1 |
| 脑穿通畸形 | 1 |
| 小头畸形 | 1 |
| 胎儿附属物异常 | 15 |
| 羊水多 | 14 |
| 单脐动脉 | 1 |
| 泌尿系统异常 | 4 |
| 双肾双肾盂 | 1 |
| 肾积水 | 1 |
| 重复肾 | 1 |
| 左肾盆腔异位肾 | 1 |
| 呼吸系统异常 | 1 |
| 隔离肺 | 1 |
| 运动系统异常 | 1 |
| 马蹄内翻足 | 1 |
| 合并2 个系统异常 | 5 |
| 神经系统异常+ 泌尿系统 | |
| 侧脑室增宽+ 多囊肾 | 1 |
| 泌尿系统异常+ 胎儿附属物异常 | |
| 右侧重复肾+ 单脐动脉+ 羊水多 | 1 |
| 神经系统异常+ 胎儿附属物异常 | |
| 室管膜下囊肿+ 单脐动脉+ 羊水多 | 1 |
| 侧脑室增宽+ 羊水多 | 1 |
| 循环系统异常+ 颅面异常 | |
| 室间隔缺损+ 颅面复合畸形 | 1 |
表4 后颅窝池畸形超声检查误诊漏诊病例情况 |
| 例序 | 年龄(岁) | 孕周(周) | 超声检查 | MRI 检查 | 合并畸形 | 确诊方式 | 妊娠结局 | ||
|---|---|---|---|---|---|---|---|---|---|
| 描述 | 结果 | 描述 | 异常类型 | ||||||
| 1 | 32 | 23+3 | 小脑及后颅窝显示清晰,小脑横径2.20 cm,后颅窝池宽0.87 cm | 胎儿左侧侧脑室增宽、右侧脑积水 | 胎儿双侧侧脑室增宽,后颅窝池位于正常值临界值。右侧侧脑室最宽17.0 mm,左侧侧脑室最宽处12.0mm,后颅窝池增宽,宽约10.2 mm | 后颅窝池增宽 | 脑积水 | 产前MRI及产后病理 | 引产 |
| 2 | 32 | 22+6 | 小脑及后颅窝显示清晰,小脑横径2.33 cm,后颅窝池宽0.91 cm | 胎儿透明隔腔隐约可显示,双侧侧脑室增宽 | 胎儿胼胝体部分缺如可能,双侧侧脑室增宽、胎儿后颅窝池位于临界值,宽约10.2 mm | 后颅窝池增宽 | 胼胝体缺如、侧脑室增宽 | 产前MRI及产后病理 | 引产 |
| 3 | 29 | 34+1 | 胎儿左、右侧侧脑室三角区内径分别为0.88 cm、0.59 cm | 胎儿未见明显异 | 胎儿左侧侧脑室稍增宽,左侧11.3mm,后颅窝池稍增宽10.5 mm | 后颅窝池增宽 | 侧脑室增宽 | 产前MRI | 分娩 |
| 4 | 34 | 36+2 | 小脑及后颅窝显示清晰,后颅窝池宽0.91 cm | 胎儿未见明显异 | 胎儿后颅窝池轻度增宽10.6 mm | 后颅窝池增宽 | 无 | 产前MRI | 分娩 |
| 5 | 33 | 33+1 | 小脑及后颅窝显示清晰,后颅窝池宽0.83 cm | 胎儿未见明显异 | 胎儿后颅窝池轻度增宽12.0 mm | 后颅窝池增宽 | 无 | 产前MRI | 分娩 |
| 6 | 37 | 28+2 | 小脑及后颅窝显示清晰,小脑横径2.62 cm,后颅窝池宽0.76 cm | 胎儿小脑横径小于孕周,左侧侧脑室位于临界值,右侧侧脑室增宽,透明隔形态及长宽比例异常 | 双侧侧脑室增宽呈泪滴状,左侧12.4mm,右侧13.7 mm,后颅窝池临界值11.9 mm,透明隔缺如,胼胝体发育不良,大脑纵裂池宽,小脑横径小(26 mm),蚓部形态正常,蛛网膜囊肿不排除,后颈部皮肤增厚 | 后颅窝池增宽 | 胼胝体缺如、侧脑室增宽 | 产前MRI及产后病理 | 引产 |
| 7 | 31 | 30+6 | 小脑形态及后颅窝宽度显示清晰,未进行测量 | 胎儿蛛网膜囊肿可能 | 后颅窝池增宽10.2 mm,右侧侧脑室较左侧饱满,透明隔腔增宽8.5mm,松果体区囊性灶 | 后颅窝池增宽 | 松果体区蛛网膜囊肿 | 产前MRI | 分娩 |
| 8 | 23 | 30+6 | 小脑形态及后颅窝宽度显示清晰,未进行测量 | 胎儿透明隔腔显示不清,双侧侧脑室增宽 | 胎儿透明隔腔缺如、胼胝体部分缺如,双侧侧脑室做2.0 mm,有12.9mm、后颅窝池增宽11.0 mm | 后颅窝池增宽 | 胼胝体缺如、侧脑室增宽 | 产前MRI及产后病理 | 引产 |
| 9 | 40 | 33+1 | 小脑形态及后颅窝宽度显示清晰,未进行测量 | 胎儿双侧侧脑室增宽 | 胎儿双侧侧脑室增宽、胎儿后颅窝池延髓池增宽,考虑蛛网膜囊肿不除外 | 后颅窝蛛网膜囊肿,后颅窝池增宽 | 侧脑室增宽 | 产前MRI检查 | 分娩 |
| 10 | 32 | 23+2 | 小脑及后颅窝显示清晰,小脑横径2.29 cm,后颅窝池宽0.61 cm | 胎儿颅后窝无回声(Blake 囊肿?) | 胎儿后颅窝池增宽11.3 mm,后颅窝蛛网膜囊肿可能 | 后颅窝蛛网膜囊肿、后颅窝池增宽 | 侧脑室增宽 | 产前MRI | 分娩 |
| 11 | 24 | 29 | 小脑及后颅窝显示清晰,后颅窝池宽0.92 cm | 胎儿颅后窝无回声(Blake 囊肿?)胎儿十二指肠稍扩张、羊水偏多 | 羊水多,后颅窝池增宽11.0 mm,蛛网膜囊肿可能 | 后颅窝蛛网膜囊肿、后颅窝池增宽 | 侧脑室增宽 | 产前MRI | 分娩 |
| 12 | 20 | 25+5 | 小脑及后颅窝显示清晰,小脑横径2.79 cm,后颅窝池宽0.78 cm | 胎儿左侧侧脑室增宽,胎儿腰椎下段及骶椎向左侧突起(半椎体不排除) | 胎儿左侧侧脑室增宽、后颅窝池增宽,小脑蚓部稍上抬,考虑Blake囊肿可能大。腰骶段脊柱弯曲,第5 腰椎半椎体可能 | Blake 囊肿 | 第5 腰椎半椎体及侧脑室增宽 | 产前MRI及产后病理 | 引产 |
| 13 | 24 | 23+6 | 小脑及后颅窝显示清晰,小脑横径2.00 cm,后颅窝池宽0.80 cm | 胎儿胼胝体发育不良可能,胸廓径线偏小,双足摇椅足 | 胎儿胼胝体缺如,小脑蚓部发育不良可能性大,延髓池增宽13.4 mm | 小脑蚓部发育不良、后颅窝池增宽 | 胼胝体缺如 | 产前MRI及产后病理 | 引产 |
| 1 |
Malinger G, Paladini D, Haratz KK, et al.Isuog practice guidelines(updated): sonographic examination of the fetal central nervous system.Part 1: performance of screening examination and indications for targeted neurosonography [J].Ultrasound Obstet Gynecol, 2020,56(3): 476-484.
|
| 2 |
Garg N, Kumar M, Rai P, et al.Relative prevalence and outcome of fetal posterior fossa abnormality [J].J Paediatr Child Health, 2023,59(1): 107-115.
|
| 3 |
D’Antonio F, Khalil A, Garel C, et al.Systematic review and metaanalysis of isolated posterior fossa malformations on prenatal ultrasound imaging (part 1): nomenclature, diagnostic accuracy and associated anomalies [J].Ultrasound Obstet Gynecol, 2016, 47(6):690-697.
|
| 4 |
Salomon LJ, Alfirevic Z, Berghella V, et al.Isuog practice guidelines(updated): performance of the routine mid-trimester fetal ultrasound scan [J].Ultrasound Obstet Gynecol, 2022, 59(6): 840-856.
|
| 5 |
Shekdar K.Posterior fossa malformations [J].Semin Ultrasound CT MRI, 2011, 32(3): 228-241.
|
| 6 |
Robinson AJ, Ederies MA.Diagnostic imaging of posterior fossa anomalies in the fetus [J].Semin Fetal and Neonatal Med, 2016, 21(5):312-320.
|
| 7 |
Venkatesan C, Kline-Fath B, Horn PS, et al.Short- and long-term outcomes of prenatally diagnosed dandy-walker malformation,vermian hypoplasia, and blake pouch cyst [J].J Child Neurol, 2021,36(12): 1111-1119.
|
| 8 |
Paladini D, Biancotto G, Della Sala F, et al.‘choroid bar’: easy-toseek marker of normal posterior fossa at 12-14 weeks’ gestation [J].Ultrasound Obstet Gynecol, 2024, 63(4): 497-501.
|
| 9 |
Friszer S, Dhombres F, Blondiaux E, et al.Patterns of detection of fetal posterior fossa anomalies: analysis of 81 cases in the second half of gestation [J].Fetal Diagn Ther, 2018, 44(4): 247-255.
|
| 10 |
Robinson AJ.Inferior vermian hypoplasia- preconception,misconception [J].Ultrasound Obstet Gynecol, 2014, 43(2): 123-136.
|
| 11 |
Milani HJF, Barreto EQDS, Ximenes RLDS, et al.Fetal posterior fossa malformations: review of the current knowledge [J].Radiologia Brasileira, 2019, 52(6): 380-386.
|
| 12 |
Pertl B, Eder S, Stern C, et al.The fetal posterior fossa on prenatal ultrasound imaging: normal longitudinal development and posterior fossa anomalies [J].Ultraschall Med, 2019, 40(6): 692.
|
| 13 |
Monteagudo A.Dandy-walker malformation [J].Am J Obstet Gynecol,2020, 223(6): B38-B41.
|
| 14 |
何冠南, 赵婧, 张玲, 等.胎儿第四脑室发育在产前超声鉴别颅后窝异常的临床应用 [J/CD].中华医学超声杂志(电子版), 2019,16(7): 504-510.
|
| 15 |
D’Antonio F, Khalil A, Garel C, et al.Systematic review and metaanalysis of isolated posterior fossa malformations on prenatal imaging(part 2): neurodevelopmental outcome [J].Ultrasound Obstet Gynecol,2016, 48(1): 28-37.
|
| 16 |
Post A, Norton ME, Monteagudo A.Blake’s pouch cyst [J].Am J Obstet Gynecol, 2020, 223(6): B47-B50.
|
| 17 |
Gandolfi Colleoni G, Contro E, Carletti A, et al.Prenatal diagnosis and outcome of fetal posterior fossa fluid collections [J].Ultrasound Obstet Gynecol, 2012, 39(6): 625-631.
|
| 18 |
张帆, 徐钟慧, 戴晴, 等.胎儿小脑延髓池增宽的产前超声与MRI对比研究 [J/OL].中华医学超声杂志(电子版), 2022, 19(3): 221-225.
|
| 19 |
Tarui T, Limperopoulos C, Sullivan NR, et al.Long-term developmental outcome of children with a fetal diagnosis of isolated inferior vermian hypoplasia [J].Arch Dis Child Fetal Neonatal Ed,2013, 99(1): F54-F58.
|
| 20 |
郭翠霞, 孙丽娟, 吴青青.Blake's陷窝囊肿的产前超声诊断进展 [J].中华超声影像学杂志, 2023, 32(9): 824-828.
|
| 21 |
Poretti A, Boltshauser E, Huisman TAGM.Pre- and postnatal neuroimaging of congenital cerebellar abnormalities [J].Cerebellum,2016, 15(1): 5-9.
|
| 22 |
郭翠霞, 吴青青, 王莉, 等.50 例胎儿颅后窝异常的超声诊断及预后分析 [J/CD].中华医学超声杂志(电子版), 2018, 15(8): 593-599.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}