
2025 , Vol. 22 >Issue 01: 55 - 61
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.01.008
甲状腺乳头状癌超声与病理测值差异及其影响因素探讨
Copy editor: 吴春凤
收稿日期: 2024-11-27
网络出版日期: 2025-04-18
基金资助
绍兴市级科技厅项目(2022A14037)
版权
Safety boundary and influencing factors of thermal ablation of papillary thyroid carcinoma
Received date: 2024-11-27
Online published: 2025-04-18
Copyright
目的
探讨甲状腺乳头状癌(PTC)超声影像与病理测值的差异性,并讨论其相关影响因素。
方法
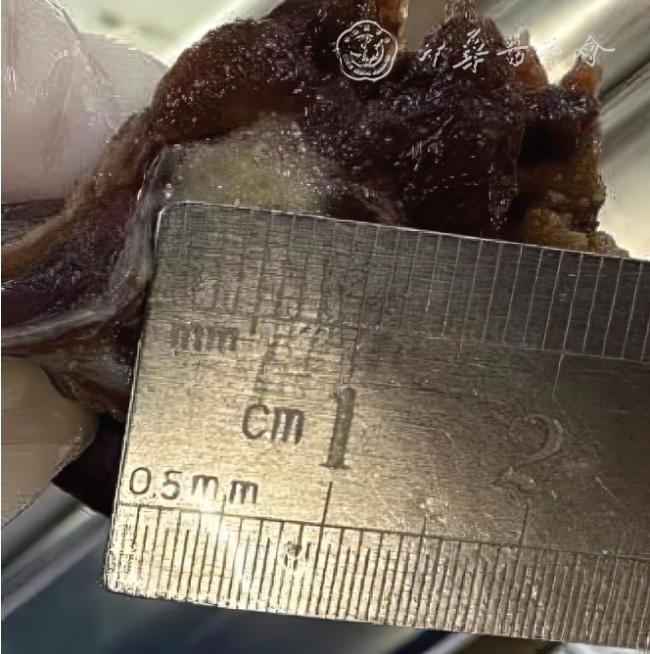
选取2023 年1 月至12 月在绍兴市上虞人民医院甲状腺外科行甲状腺部分或全部切除的患者,病理证实为单侧叶单发的PTC。采集病灶的超声影像、大体标本、显微镜下的大小,包括左右径和上下径。采用Kruskal-Wallis H 检验比较3 种测量方式下癌灶大小的差异,对镜下病理测量结果与超声测量结果差异的影响因素行Logistic 多因素回归分析,采用χ2 检验分别比较筛选出的影响因素的发生情况。
结果
虽然3 种测量方式病灶大小整体差异没有统计学意义(P>0.05),但显微镜下测值较超声偏大者有21 个(30.0%,21/69),显微镜下病灶测量范围大于超声影像的差值介于:0.2 ~2.2 mm(左右径)、0.1 ~0.9 mm(上下径)之间。Logistic 多因素回归分析显示,病灶内钙化及病灶周边高回声声晕是镜下病理范围偏大的保护因素(β=-2.662,P=0.039;β=-2.883,P=0.015)。镜下病理测值偏大的病灶,其内钙化和周边高回声声晕的比例更高(15/21 vs 19/48,χ²=5.927,P=0.015;11/18 vs 8/51,χ²=9.581,P=0.001)。
结论
PTC 部分病例的病理测值范围大于超声,提示病灶的主瘤体周边存在超声影像无法显示的微小癌灶;超声影像若显示微钙化或高回声声晕,超声影像测值有可能小于镜下病理测值。
龚月江 , 王倩 , 李世岩 , 黄昌文 , 陈锦锦 , 任伟丽 , 陈椿林 , 叶莉媛 . 甲状腺乳头状癌超声与病理测值差异及其影响因素探讨[J]. 中华医学超声杂志(电子版), 2025 , 22(01) : 55 -61 . DOI: 10.3877/cma.j.issn.1672-6448.2025.01.008
Objective
To explore the differences between ultrasound imaging and pathological measurements of papillary thyroid carcinoma (PTC), and to discuss the related influencing factors.
Methods
Patients who underwent partial or total thyroidectomy in the Department of Thyroid Surgery of Shangyu People’s Hospital of Shaoxing from January 2023 to December 2023 were selected, and their pathology confirmed that they had single-occurrence papillary thyroid carcinoma (PTC) in a single thyroid lobe.The sizes of cancer lesions on ultrasonic images, on gross specimens, and under the microscope were collected.The Kruskal-Wallis H test was used to compare the differences in the sizes of the cancerous lesions measured by the three measurement methods.Logistic multivariate regression analysis was performed on the influencing factors of the differences between the pathological measurement results under the microscope and the ultrasonic measurement results.The chi-square test was used to compare the selected influencing factors,respectively.
Results
There was no significant difference among the three measurement methods as a whole of the sizes of the cancerous lesions (P>0.05), but there were still 21 cases (30.0%, 21/69) that showed larger values under microscopy.The differences between microscopic lesion measurements and ultrasound imaging ranged as follows: transverse diameter 0.2-2.2 mm and longitudinal diameter 0.1-0.9 mm.Logistic multiple regression analysis showed that calcification within the lesion and hyperechoic halos around the lesion were protective factors for a larger pathological range on microscopic examination (β=-2.662, P=0.039;β=-2.883, P=0.015).The chi-square test revealed that lesions with high pathological values had a higher probability of internal calcification and peripheral hyperechoic halos (15/21 vs 19/48, χ²=5.927, P=0.015;11/18 vs 8/51, χ²=9.581, P=0.001).
Conclusion
The pathological extent exceeded ultrasonographic measurements in some PTC cases, suggesting that there are small cancerous lesions around the main tumor body that cannot be displayed by ultrasound imaging.If ultrasound imaging shows microcalcifications or hyperechoic halos, the ultrasound measurement may be smaller than the pathological measurement.
Key words: Papillary thyroid carcinoma; Ultrasound; Safety boundary; Halo; Pathology
表1 69 个甲状腺乳头状癌病灶3 种测量方式的结果比较[mm,M(QR)] |
| 测量方式 | 上下径 | 左右径 |
|---|---|---|
| 超声 | 6.8(2.3,19.1) | 5.8(2.6,12.1) |
| 标本 | 6.1(1.0,17.0) | 5.3(1.0,12.0) |
| 显微镜下 | 5.8(0.8,15.2) | 5.1(0.7,12.4) |
| H 值 | 3.239 | 3.310 |
| P 值 | 0.198 | 0.191 |
表2 甲状腺乳头状癌病灶边界镜下病理测值与超声测值不同的多因素Logistic 回归分析 |
| 参数 | β 值 | SE 值 | Wald 值 | P 值 | Exp(B) 值 | 95%CI |
|---|---|---|---|---|---|---|
| 性别 | -0.649 | 1.239 | 0.274 | 0.601 | 0.523 | 0.046 ~ 5.931 |
| 年龄 | 0.014 | 0.039 | 0.129 | 0.719 | 1.014 | 0.939 ~ 1.095 |
| 家族史 | 16.896 | 18 081.679 | 0.000 | 0.999 | 21 779 534.353 | 0.000 |
| 个人史 | 0.882 | 1.200 | 0.540 | 0.462 | 2.416 | 0.230 ~ 25.390 |
| 甲状腺功能 | 0.920 | 0.817 | 1.268 | 0.260 | 2.508 | 0.506 ~ 12.432 |
| 甲状腺球蛋白 | 0.372 | 0.852 | 0.191 | 0.662 | 1.451 | 0.273 ~ 7.705 |
| 超声测量结节大小 | -0.788 | 0.756 | 1.087 | 0.297 | 0.455 | 0.103 ~ 2.002 |
| 生长方式 | 21.450 | 9224.391 | 0.000 | 0.998 | 2 067 955 382.041 | 0.000 |
| 钙化 | -2.662 | 1.292 | 4.243 | 0.039 | 0.070 | 0.006 ~ 0.879 |
| 边缘 | -0.095 | 1.438 | 0.004 | 0.947 | 0.909 | 0.054 ~ 15.222 |
| 近包膜 | 0.938 | 1.854 | 0.256 | 0.613 | 2.556 | 0.067 ~ 96.790 |
| 高回声声晕 | -2.883 | 1.184 | 5.931 | 0.015 | 0.056 | 0.006 ~ 0.570 |
表3 甲状腺乳头状癌病灶边界的病理与超声测量结果中钙化和高回声声晕出现情况(个) |
| 测值结果 | 病灶数 | 钙化 | 高回声声晕 | ||
|---|---|---|---|---|---|
| 有 | 无 | 有 | 无 | ||
| 超声影像测值偏大 | 48 | 19 | 29 | 8 | 40 |
| 显微镜下病理测值偏大 | 21 | 15 | 6 | 11 | 10 |
| χ 2 值 | 5.927 | 9.581 | |||
| P 值 | 0.015 | 0.001 | |||
| 1 |
Sung H, Ferlay J, Siegel RL, et al.Global Cancer Statistics 2020:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries [J].CA Cancer J Clin, 2021, 71(3): 209-249.
|
| 2 |
殷德涛, 鞠定吾.热消融在低危甲状腺微小乳头状癌治疗中的应用现状 [J].国际外科学杂志, 2022, 49(2): 73-78.
|
| 3 |
Haugen BR, Alexander EK, Bible KC, et al.2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cance [J].Thyroid, 2016, 26(1): 1-133.
|
| 4 |
Gharib H, Papini E, Garber JR, et al.American Association Of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guideline for cilinical practice for the diagnosis and management of thyroid nodules-2016 update [J].Endocr Pract, 2016, 22(Suppl 1): 1-60.
|
| 5 |
中华医学会内分泌学分会, 中华医学会外科学分会内分泌学组,中国抗癌协会头颈肿瘤专业委员会, 等.甲状腺结节和分化型甲状腺癌诊治指南 [J/CD].中华核医学与分子影像杂志(电子版),2013, 33(2): 96-115.
|
| 6 |
章建全, 陈红琼, 闫磊, 等.对甲状腺结节细针穿刺有关问题的新思考 [J/OL].中华医学超声杂志(电子版), 2023, 20(10): 1007-1011.
|
| 7 |
中国医师协会超声医师分会.甲状腺微小乳头状癌热消融诊疗指证专家共识 [J/CD].中华医学超声杂志(电子版), 2019, 16(8): 571-574.
|
| 8 |
高明, 葛明华, 嵇庆海, 等.甲状腺微小乳头状癌诊断与治疗中国专家共识(2016 版) [J].中国肿瘤临床, 2016, 43(10): 405-411.
|
| 9 |
Lloyd RV, Osamura RY, Kloppel G, et al.WHO classification of tumours: pathology and genetics of tumours of endocrineorgans [M].4th ed.Lyon: IARC Press, 2017(10): 65-142.
|
| 10 |
许敏, 赵齐羽, 蒋天安.热消融在甲状腺癌治疗中的应用现状与争议 [J].中华超声影像学杂志, 2021, 30(11): 1007-1012.
|
| 11 |
颜燕煌, 林晶, 高子斌, 等.甲状腺微小乳头状癌144 例热消融范围探讨 [J].肿瘤学杂志, 2019, 25(10): 924-925.
|
| 12 |
Deveci MS, Deveci G, LiVolsi VA, et al.Concordance between thyroid nodule sizes measured by ultrasound and gross pathology examination:effect on patient management [J].Diagn Cytopathol,2007, 35(9): 579-583.
|
| 13 |
Bachar G, Buda I, Cohen M, et al.Size discrepancy between sonographic and pathological evaluation of solitary papillary thyroid carcinoma [J].Eur J Radiol, 2013, 82(11): 1899-1903.
|
| 14 |
Yoon YH, Kwon KR, Kwak SY, et al.Tumor size measured by preoperative ultrasonography and postoperative pathologic examination in papillarythyroid carcinoma:relative differences according to size, calcification and coexisting thyroiditis [J].Eur Arch Otorhinolaryngol, 2014, 271(5): 1235-1239.
|
| 15 |
丁金旺, 韩志江, 张卧, 等.甲状腺结节超声纵横比与大体组织纵横比的对照研究 [J].中国临床医学影像杂志, 2016, 27(5): 337-340.
|
| 16 |
王颖, 丁金旺, 韩志江, 等.超声检查和病理测量甲状腺乳头状癌肿瘤大小的对比研究[J].中国耳鼻咽喉头颈外科, 2017, 24(3):149-152.
|
| 17 |
Choi SH, Kim EK, Kwak JY, et al.Interobserver and intraobserver variations in ultrasound assessment of thyroid nodules [J].Thyroid,2010, 20(2): 167-172.
|
| 18 |
Kshithi K, Kamboj V, Sreedharan S, et al.Effect of formalin fixation on tumour size and margins in head and neck cancer specimens [J].Acta Otorhinolaryngol Ital, 2022, 42(5): 434-440.
|
| 19 |
王万菊, 张冬, 刘放, 等.微小钙化及纵横比大于1 在TI-RADS 4 类甲状腺结节中的诊断价值 [J].中国现代普通外科进展, 2022,25(5): 356-361.
|
| 20 |
王帅, 徐辉雄, 徐军妹, 等.甲状腺结节微钙化、粗大钙化及环状钙化与甲状腺癌的相关性分析 [J].影像诊断与介入放射学, 2015,24(3): 212-215.
|
| 21 |
Oh EM, Chung YS, Song WJ, et al.The pattern and significance of the calcifications of papillary thyroid microcarcinoma presented in preoperative neck ultrasonography [J].Ann Surg Treat Res, 2014,86(3): 115-121.
|
| 22 |
Pyo JS, Kang G, Kim DH, et al.The prognostic relevance of psammoma bodies and ultrasonographic intratumoral calcifications in papillary thyroid carcinoma [J].World J Surg, 2013, 37(10): 2330-2335.
|
| 23 |
李晶, 姜罗, 史铁梅.乳腺癌超声恶性晕病理基础 [J].中华超声影像学杂志, 2012, 21(9): 787-790.
|
| 24 |
吴剑, 杨湛.肿瘤浸润前沿细胞的生物学特性 [J].医学综述, 2007,13(13): 986-988.
|
| 25 |
白艳花, 薛卫成.甲状腺乳头状癌的组织学特点、分子标志物表达与临床预后的关系 [J].中华病理学杂志, 2014, 43(5): 341-343.
|
| 26 |
Jin H, Yan H, Tang H, et al.Internal spreading of papillary thyroid carcinoma: a case report and systemic review [J].Case Rep Endocrinol, 2018, 2018: 7618456.
|
| 27 |
Pancer J, Mitmaker E, Ajise O, et al.A thyroid gland with over 30 foci of papillary thyroid carcinoma with activating BRAF V600E mutation[J].Endocrinol Diabetes Metab Case Rep, 2019, 2019: 19-0006.
|
| 28 |
Lei Y, Feng S, Yu Q, et al.Conventional papillary thyroid carcinoma with intraglandular lymphatic dissemination shows more aggressive features [J].Jpn J Clin Oncol, 2022, 52(11): 1311-1320.
|
| 29 |
Fang H, Si Y, Wang C, et al.Diffuse intrathyroidal dissemination of papillary thyroid carcinoma with no stromal fibrosis at presentation: A pattern of aggressive differentiated thyroid carcinoma [J].Pathol Res Pract, 2021, 224: 153510.
|
/
| 〈 |
|
〉 |


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}