
2025 , Vol. 22 >Issue 01: 79 - 85
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.01.011
多模态便携超声引导改良穿刺法制作髂动脉破裂出血模型
Copy editor: 吴春凤
收稿日期: 2024-10-11
网络出版日期: 2025-04-18
基金资助
国家重点研发计划(2022YFB4703500)
版权
Establishment of a pig model of iliac artery rupture and hemorrhage by improved multimodal portable ultrasound-guided puncture method
Received date: 2024-10-11
Online published: 2025-04-18
Copyright
目的
探讨多模态便携超声引导下改良穿刺法制备猪髂动脉破裂出血模型的可行性及稳定性。
方法
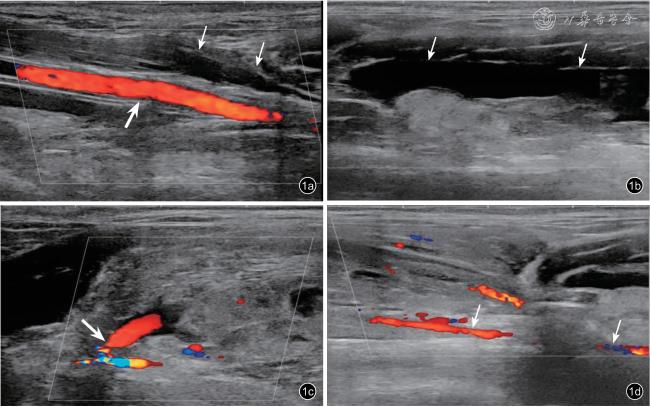
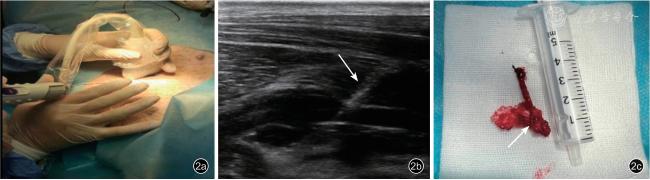
实验巴马小型猪6 只,体质量35~45 kg。在超声引导下于右侧颈内静脉置入静脉导管用于术中补液及麻醉维持,同时经颈总动脉穿刺放置PiCCO 管,用于监测基础生命体征(血压、心率、体温)。在便携超声引导下对髂动脉穿刺靶点周围注入20 ml 肝素与生理盐水混合液体(12 500 单位肝素钠+100 ml 生理盐水),使其局部肝素化,然后在便携超声实时引导下使用一次性活检针对猪髂动脉进行穿刺建模。连续记录建模前后实验猪血压、心率及体温。于建模后即刻(0 min)、10 min、20 min、30 min,运用多模态便携超声[灰阶超声、彩色多普勒超声(CDUS)、频谱多普勒超声(PW)、超声造影(CEUS)、微血流成像(MFI)]对髂动脉活动性出血进行定性、定位诊断,并评估其诊断效能;同时运用多模态便携超声对建模前后髂动脉穿刺部位远端1~1.5 cm 处管腔横截面积及血流速度进行监测。出血30 min 后处死动物并进行解剖,采集髂动脉血管标本。采用配对t 检验比较建模前后基础生命体征和动脉血流动力学指标的差异;采用χ2 检验及Bonferroni 校正法比较不同影像模式的诊断效能。
结果
6 只实验动物均一次性建模成功。建模后,收缩压、舒张压、平均动脉压、体温均较建模前降低[(100.33±4.41)mmHg vs (146.17±5.19)mmHg,(70.33±4.97)mmHg vs (115.67±16.51)mmHg,(80.00±2.89)mmHg vs (118.33±3.88)mmHg,(36.45±0.38) ℃ vs(37.41±0.41) ℃],心率较建模前增快[(111.50±2.74)次/min vs (79.83±6.65)次/min],差异均具有统计学意义(t=22.469、6.657、17.068、4.503、-10.162,P<0.001、=0.001、=0.001、=0.006、<0.001)。建模后0 min、10min 时,CEUS 联合MFI、CDUS、CEUS、MFI 对髂动脉活动性出血的定性及定位诊断差异无统计学意义(P 均>0.05);建模后20 min 时,CEUS 联合MFI 诊断髂动脉活动性出血及定位出血部位的效能高于CDUS,差异具有统计学意义(P=0.015),但与CEUS、MFI 的诊断差异无统计学意义(P>0.05);建模后30 min 时,CEUS 联合MFI 诊断髂动脉活动性出血及定位出血部位的效能高于CDUS、MFI,差异具有统计学意义(P=0.015、0.015),但与CEUS 的诊断差异无统计学意义(P>0.05)。同时,髂动脉穿刺口远端管腔内径横截面积较建模前减小[(0.13±0.08)cm2vs(0.38±0.17)cm2],髂动脉穿刺口远端收缩期血流速度、舒张期血流速度、平均血流速度、阻力指数、搏动指数较建模前减低[(65.24±15.76)cm/s vs (115.53±11.25)cm/s,(11.23±5.45)cm/s vs(-21.36±2.45)cm/s,(21.95±11.36)cm/s vs (75.27±12.35)cm/s,(0.74±0.16) vs (1.08±0.25),(1.13±0.28) vs (1.81±0.36)],差异均具有统计学意义(t=8.510、-17.608、11.137、8.470、7.605,P<0.001、<0.001、<0.001、<0.001、=0.001)。解剖后髂动脉大体标本可显示穿刺破裂口。
结论
应用多模态便携超声引导局部肝素化髂动脉穿刺出血建模准确性、稳定性好,并可实时准确评估髂动脉出血状态,为交界部位血管创伤出血的救治研究提供了动物模型依据。
高农 , 豆梦杰 , 王冬丽 , 马秀珠 , 吕发勤 . 多模态便携超声引导改良穿刺法制作髂动脉破裂出血模型[J]. 中华医学超声杂志(电子版), 2025 , 22(01) : 79 -85 . DOI: 10.3877/cma.j.issn.1672-6448.2025.01.011
Objective
To explore the feasibility and stability of an improved puncture method under multimodal portable ultrasound guidance to prepare a pig iliac artery rupture and bleeding model.
Methods
Six Bama miniature pigs (35-45 kg) were utilized.Under ultrasound guidance, a venous catheter was inserted into the right internal jugular vein for intraoperative fluid administration and anesthesia maintenance.A PiCCO catheter was placed via the common carotid artery to monitor baseline vital signs (blood pressure, heart rate, and body temperature).A heparinized saline solution (12500 units heparin sodium +100 ml saline) was injected around the iliac artery puncture target under portable ultrasound guidance to achieve local heparinization.Subsequently,a disposable biopsy needle was used to puncture the iliac artery under real-time ultrasound guidance for model establishment.Vital signs were continuously recorded before and after modeling.At 0, 10, 20, and 30 minutes post-modeling, multiple portable ultrasound modalities [grayscale ultrasound, color Doppler ultrasound (CDUS),spectral Doppler ultrasound (PW), contrast-enhanced ultrasound (CEUS), and microvascular flow imaging (MFI)]were employed for qualitative and localization diagnosis of active iliac artery hemorrhage, with diagnostic efficacy evaluated.Additionally, cross-sectional area and hemodynamic parameters (peak systolic velocity (PSV), enddiastolic velocity (EDV), mean velocity (Vmean), resistance index (RI), and pulsatility index (PI)) at 1-1.5 cm distal to the puncture site were monitored.Animals were euthanized after 30 minutes for anatomical validation.Paired t-tests were used to compare pre- and post-modeling hemodynamic parameters.The chi-square test (χ2 test) and Bonferroni correction method were used to compare the diagnostic efficacy of different imaging modalities between groups.
Results
The modeling in all the six experimental animals was successfully completed at one time.After modeling, the systolic blood pressure, diastolic blood pressure, mean arterial pressure, and body temperature were all lower than those before modeling [(100.33±4.41) mmHg vs (146.17±5.19) mmHg, (70.33±4.97)mmHg vs (115.67±16.51) mmHg, (80.00±2.89) mmHg vs (118.33±3.88) mmHg, and (36.45±0.38)°C vs(37.41±0.41)°C, respectively], and the heart rate was faster than that before modeling [(111.50±2.74) beats/min vs (79.83±6.65) beats/min]; all the differences were statistically significant (t=22.469, 6.657, 17.068, 4.503,and -10.162, P<0.001, =0.001, =0.001, =0.006, and <0.001, respectively).At 0 minutes and 10 minutes after modeling, there were no statistically significant differences in the qualitative and localization diagnosis of active iliac artery bleeding among contrast-enhanced ultrasound (CEUS) combined with microflow imaging (MFI), color Doppler ultrasound (CDUS), CEUS, and MFI (all P>0.05).At 20 minutes after modeling, the efficacy of CEUS combined with MFI in diagnosing active iliac artery bleeding and locating the bleeding site was significantly higher than that of CDUS (P=0.015), but there were no statistically significant differences when compared with CEUS and MFI (P>0.05).At 30 minutes after modeling, the efficacy of CEUS combined with MFI in diagnosing active iliac artery bleeding and locating the bleeding site was significantly higher than that of CDUS and MFI (P=0.015 and 0.015, respectively), but there was no statistically significant difference when compared with CEUS (P>0.05).Meanwhile, the cross-sectional area of the diameter at the distal end of the iliac artery puncture site was smaller than that before modeling [(0.13±0.08)cm² vs (0.38±0.17)cm²], and the systolic blood flow velocity, diastolic blood flow velocity, mean blood flow velocity, resistance index, and pulsatility index at the distal end of the iliac artery puncture site were lower than those before modeling [(65.24±15.76)cm/s vs (115.53±11.25)cm/s, (11.23±5.45)cm/s vs (-21.36±2.45)cm/s, (21.95±11.36)cm/s vs (75.27±12.35)cm/s, (0.74±0.16) vs (1.08±0.25), and(1.13±0.28) vs (1.81±0.36), respectively]; all the differences were statistically significant (t=8.510, -17.608,11.137, 8.470, and 7.605, P<0.001, <0.001, <0.001, <0.001, and =0.001, respectively).The puncture rupture site could be shown in the gross specimens of the iliac artery after dissection.
Conclusion
The modeling of local heparinized iliac artery puncture bleeding guided by multimodal portable ultrasound is accurate and stable, and can be used to accurately evaluate the bleeding status of the iliac artery in real time, providing an animal model basis for the treatment of vascular trauma bleeding at the junction.
 ±s 表示,采用t 检验比较建模前后的差异;不同影像模式诊断效能为计数资料,以频数表示,组间比较采用χ2 检验及Bonferroni 校正法,以P<0.05 为差异有统计学意义。
±s 表示,采用t 检验比较建模前后的差异;不同影像模式诊断效能为计数资料,以频数表示,组间比较采用χ2 检验及Bonferroni 校正法,以P<0.05 为差异有统计学意义。表1 建模前后6 只巴马小型猪基础生命体征指标比较( |
| 时间 | 体温(℃) | 收缩压(mmHg) | 舒张压(mmHg) | 平均动脉压(mmHg) | 心率(次/min) |
|---|---|---|---|---|---|
| 建模前 | 37.41±0.41 | 146.17±5.19 | 115.67±16.51 | 118.33±3.88 | 79.83±6.65 |
| 建模后 | 36.45±0.38 | 100.33±4.41 | 70.33±4.97 | 80.00±2.89 | 111.50±2.74 |
| t 值 | 4.503 | 22.469 | 6.657 | 17.068 | -10.162 |
| P 值 | 0.006 | < 0.001 | 0.001 | 0.001 | < 0.001 |
注:1 mmHg=0.133 kPa |
表2 建模前后6 只巴马小型猪髂动脉血流动力学指标比较( |
| 时间 | 管腔横截面积(cm2) | PSV(cm/s) | EDV(cm/s) | Vmean(cm/s) | RI | PI |
|---|---|---|---|---|---|---|
| 建模前 | 0.38±0.17 | 115.53±11.25 | -21.36±2.45 | 75.27±12.35 | 1.08±0.25 | 1.81±0.36 |
| 建模后 | 0.13±0.08 | 65.24±15.76 | 11.23±5.45 | 21.95±11.36 | 0.74±0.16 | 1.13±0.28 |
| t 值 | 6.080 | 8.510 | -17.608 | 11.137 | 8.470 | 7.605 |
| P 值 | 0.002 | < 0.001 | < 0.001 | < 0.001 | < 0.001 | 0.001 |
注:PSV 为收缩期血流速度,EDV 为舒张期血流速度,Vmean 为平均血流速度,RI 为阻力指数,PI 为搏动指数 |
表3 不同影像模式对髂动脉穿刺口定位及出血的诊断效能(只) |
| 影像模式 | 只数 | 0 min | 10 min | 20 min | 30 min |
|---|---|---|---|---|---|
| CDUS | 6 | 6 | 2 | 1 | 1 |
| CEUS | 6 | 6 | 4 | 3 | 2 |
| MFI | 6 | 6 | 4 | 2 | 1 |
| CEUS 联合MFI | 6 | 6 | 6 | 6a | 6ab |
| χ 2 值 | - | 5.778 | 9.286 | 11.136 | |
| P 值 | 1.000 | 0.143 | 0.015 | 0.015 |
注:CDUS 为彩色多普勒超声,CEUS 为超声造影,MFI 为微血流成像。-为组间完全没有差异,无统计值。a 与CDUS 比较,差异具有统计学意义(P 均=0.015)。b 与MFI 比较,差异具有统计学意义(P=0.015) |
| 1 |
Chang R, Fox EE, Greene TJ, et al.Multicenter retrospective study of non-compressible torso hemorrhage: anatomic locations of bleeding and comparison of endovascular versus open approach [J].Trauma Acute Care Surg, 2017, 83(1): 11-18.
|
| 2 |
Smith Shane A, McAlister VC, Dubois L, et al.Managing junctional haemorrhage in the combat environment [J].BMJ Mil Health, 2021,167: 114-117.
|
| 3 |
Kotwal RS, Butler FK Jr.Junctional hemorrhage control for tactical combat casualty care [J].Wilderness Environ Med, 2017, 28(2S):S33-S38.
|
| 4 |
Kheirabadi BS, Terrazas IB, Miranda N, et al.Physiological consequences of abdominal aortic and junctional tourniquet (AAJT)application to control hemorrhage in a swine model [J].Shock, 2016,46(3 Suppl 1): 160-166.
|
| 5 |
Arnaud F, Parreño-Sadalan D, Tomori T, et al.Comparison of 10 hemostatic dressings in a groin transection model in swine [J].Trauma,2009, 67(4): 848-855.
|
| 6 |
黄钰清, 吴盛正, 陈祥慧, 等.超声引导下髂动脉破裂出血模型的建立 [J/OL].中华医学超声杂志(电子版), 2021, 18(4): 407-411.
|
| 7 |
Kotwal RS, Butler FK Jr, Gross K, et al.Management of junctional hemorrhage in tactical combat casualty care: TCCC guidelines?Proposed change 13-03 [J].J Spec Oper Med, 2013, 13(4): 85-93.
|
| 8 |
Smith S, White J, Wanis KN, et al.The effectiveness of junctional tourniquets: a systematic review and meta-analysis [J].J Trauma Acute Care Surg, 2018, 86(3): 532-539.
|
| 9 |
Handford C, Parker PJ.The potential use of the abdominal aortic junctional Tourniquet® in a military population: a review of requirement,effectiveness, and usability [J].J Spec Oper Med, 2020, 19(4): 74-79.
|
| 10 |
董科, 高明, 楚雪欣, 等.美军战术战伤救治指南止血器材研究 [J].中华灾害救援医学, 2022, 10(5): 253-257.
|
| 11 |
Kotwal RS, Butler FK, Edgar EP, et al.Saving lives on the battlefield:a joint trauma system review of pre-hospital trauma care in combined joint operating area ? Afghanistan (CJOA-A) executive summary [J].J Spec Oper Med, 2013, 13(1): 77-85.
|
| 12 |
Schechtman DW, Kauvar DS, De Guzman R, et al.Abdominal aortic and junctional tourniquet versus zone III resuscitative endovascular balloon occlusion of the aorta in a swine junctional hemorrhage model[J].J Trauma Acute Care Surg, 2020, 88(2): 292-297.
|
| 13 |
Pratt 3rd GA, Kishman AJ, Glaser JJ, et al.Evaluation of hemostatic devices in a randomized porcine model of junctional hemorrhage and 72-hour prolonged field care [J].J Trauma Acute Care Surg, 2023,96(2): 256-264.
|
| 14 |
张贺, 金海, 李雪华, 等.巴马小型猪失血性休克模型建立及评价[J].临床军医杂志, 2021, 49(9): 971-973, 977.
|
| 15 |
丁付燕, 吕志前, 王瑾晔, 等.新型地塞米松-肝素双涂层支架在小型猪动脉损伤模型中预防支架内再狭窄的实验研究 [J].国际心血管病杂志, 2011, 38(1): 52-55.
|
| 16 |
Tagliati C, Argalia G, Graziani B, et al.Contrast-enhanced ultrasound in the evaluation of splenic injury healing time and grade [J].Radiol Med, 2018, 124(3): 163-169.
|
| 17 |
Lv F, Tang J, Luo Y, et al.Contrast-enhanced ultrasound imaging of active bleeding associated with hepatic and splenic trauma [J].Radiol Med, 2011, 116(7): 1076-1082.
|
| 18 |
Piskunowicz M, Stefanowicz J, Batko T, et al.Contrast-enhanced ultrasound of adrenal hemorrhage: a helpful problem solving tool [J].Med Ultrason, 2022, 24(3): 284-289.
|
| 19 |
Roberto C, Giulia P, Mariasole M, et al.New microvascular ultrasound techniques: abdominal applications [J].Radiol Med, 2023, 128(9):1023-1034.
|
| 20 |
Vora KP, Kumar A, Krishnam MS, et al.Microvascular obstruction and intramyocardial hemorrhage in reperfused myocardial infarctions:pathophysiology and clinical insights from imaging [J].JACC Cardiovasc Imaging, 2024, 17(7): 795-810.
|
| 21 |
Naritaka H, Ishikawa M, Terao S, et al.Ultrasonographic superb microvascular imaging for emergency surgery of intracerebral hemorrhage [J].J Clin Neurosci, 2020, 75: 206-209.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}