
2025 , Vol. 22 >Issue 04: 337 - 347
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.04.009
自动乳腺超声联合临床病理特征预测Luminal B 型乳腺癌术后复发风险的临床研究
Copy editor: 汪荣
收稿日期: 2025-01-22
网络出版日期: 2025-06-09
基金资助
国家自然科学基金面上资助项目(82071934、82471991)西京医院助推项目创新医学研究专项(XJZT25CX03)
版权
Prediction of postoperative recurrence risk of luminal B breast cancer using automated breast ultrasound combined with clinicopathological features: a clinical study
Received date: 2025-01-22
Online published: 2025-06-09
Copyright
目的
探讨基于术前自动乳腺超声(ABUS)图像联合临床病理特征建立的Luminal B 型乳腺癌术后复发风险预测模型的临床价值。
方法
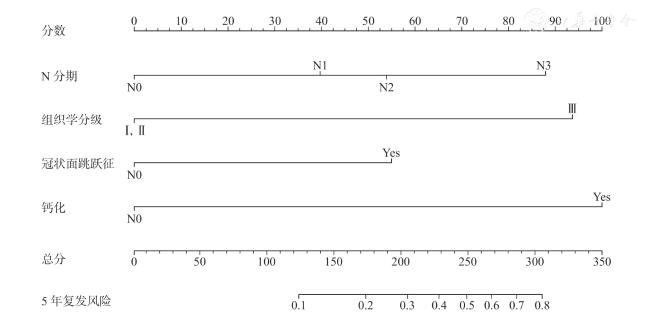
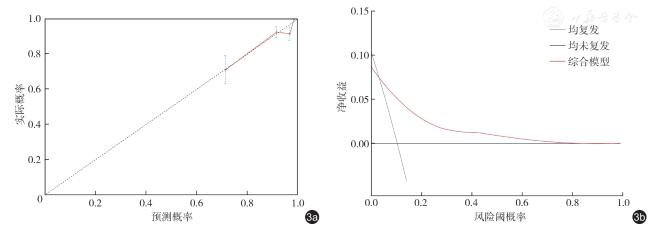
回顾性收集2016 年1 月至2019 年12 月于西京医院确诊并接受乳腺癌手术治疗的293 例Luminal B 型乳腺癌女性患者,所有患者在术前均接受ABUS 检查。根据患者是否复发将患者分为复发组与未复发组,比较两组间临床病理特征及ABUS图像特征的差异,将单因素分析差异有统计学意义的因素纳入多因素Cox 回归分析,确定Luminal B 型患者术后复发的独立风险因素,根据独立风险因素构建临床病理模型、ABUS 模型及综合模型3 种预测模型,并绘制3 年和5 年的ROC 曲线评估各模型预测性能,通过DeLong 检验比较3 种模型的ROC 曲线下面积(AUC)。选择性能最佳的模型绘制列线图,采用Bootstrap 法对最佳模型进行内部验证,绘制校准曲线、决策曲线评估最佳模型的效能。绘制不同复发风险因素特征患者的Kaplan-Meier 生存曲线,并进行Log-rank 检验。
结果
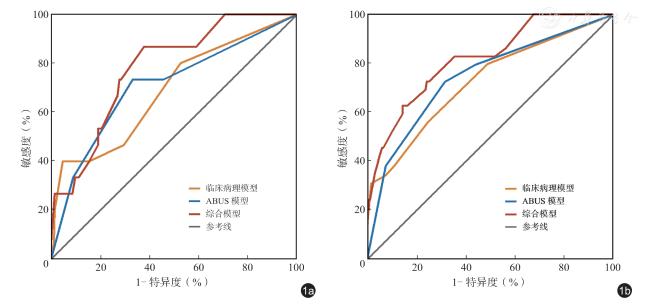
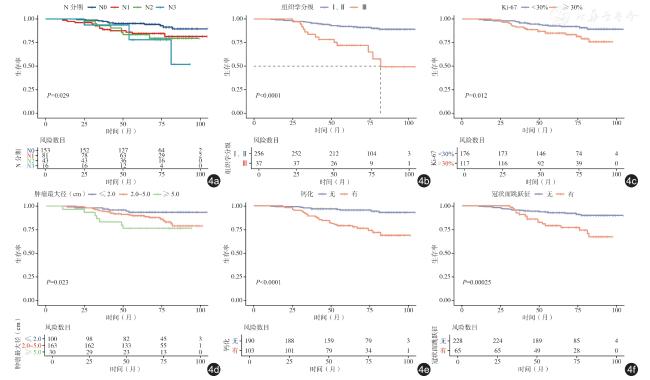
293 例Luminal B 型乳腺癌术后患者,在中位随访时间为68 个月的随访中,36 例患者发生复发,术后复发率为12.3%(36/293)。未复发组与复发组之间N 分期、组织学分级、Ki-67 表达、肿瘤最大径、钙化以及冠状面跳跃征差异均有统计学意义(P<0.05);经多因素Cox 回归分析显示,N3 级(HR=3.762,95%CI:1.147 ~12.337,P=0.029)、组织学分级Ⅲ级(HR=3.558,95%CI:1.631 ~7.759,P=0.001)、钙化(HR=4.066,95%CI:1.888 ~8.757,P<0.001)与冠状面跳跃征(HR=2.178,95%CI:1.064 ~4.460,P=0.033)是Luminal B 型患者复发的独立风险因素。建立的3 种模型的一致性指数(C-index)分别为临床病理模型0.687、ABUS 模型0.734、综合模型0.791。绘制3 种模型3 年与5 年的ROC 曲线,结果显示,临床病理模型、ABUS 模型和综合模型3 年AUC 分别为0.688、0.707、0.779,5 年AUC 分别为0.724、0.745、0.819;DeLong 检验结果显示综合模型5 年AUC 显著高于临床病理模型和ABUS 图像模型(Z=2.759、2.13,P<0.05)。内部验证结果显示综合模型稳定性较好(C-index=0.788);校准曲线显示,综合模型的校准曲线贴近理想曲线;临床决策曲线显示,在3.0%~81.0%广泛阈概率范围内,综合模型具有较高的临床净收益。生存分析结果显示,术后患者的3 年和5 年累积生存率分别为92.38%和88.47%,不同的N 分期、不同组织学分级、不同Ki-67 表达、不同肿瘤最大径、有无钙化、有无冠状面跳跃征患者的累积生存率之间差异均有统计学意义(P<0.05)。
结论
ABUS 图像联合临床病理特征建立的预测模型具有较好的性能,该模型为预测Luminal B 型乳腺癌术后复发风险提供了一种高效、准确且经济的新方法,有助于临床医师评估复发风险以及制定个性化随访方案。
关键词: 自动乳腺超声; 乳腺癌; Luminal B 型; 复发风险; 预测模型
明昊 , 宋宏萍 , 白誉誉 , 党晓智 , 赵阳 , 程燕妮 , 王琪 , 肖迎聪 . 自动乳腺超声联合临床病理特征预测Luminal B 型乳腺癌术后复发风险的临床研究[J]. 中华医学超声杂志(电子版), 2025 , 22(04) : 337 -347 . DOI: 10.3877/cma.j.issn.1672-6448.2025.04.009
Objective
To evaluate the clinical value of a postoperative recurrence risk prediction model for luminal B breast cancer based on preoperative automated breast ultrasound (ABUS) images combined with clinicopathological features.
Methods
A retrospective analysis was conducted on 293 female patients with luminal B breast cancer who were diagnosed and underwent surgical treatment at Xijing Hospital from January 2016 to December 2019.All patients underwent preoperative ABUS examination.Patients were categorized into a recurrence group and a non-recurrence group based on their recurrence status.Differences in clinicopathological characteristics and ABUS imaging features between the two groups were compared.Factors identified to have statistical significance in the univariate analysis were included in a multivariate Cox regression model to identify independent risk factors for postoperative recurrence in luminal B breast cancer patients.Based on the identified independent risk factors, three predictive models were constructed: a clinicopathological model, an ABUS model,and a combination model.Receiver operating characteristic (ROC) curves were generated to assess the predictive performance of each model.The area under the ROC curve (AUC) values of the three models were compared using the DeLong test.The model with the best performance was used to develop a nomogram, and its internal validation was performed using the Bootstrap method.Calibration curves and decision curve analysis (DCA) were used to evaluate the efficacy of the optimal model.Kaplan-Meier survival curves stratified by different recurrence risk factors were constructed, and the differences were tested using the Log-rank test.
Results
Among the 293 postoperative luminal B breast cancer patients, 36 experienced recurrence during a median follow-up of 68 months,resulting in a postoperative recurrence rate of 12.3% (36/293).Significant differences were observed between the recurrence and non-recurrence groups in N stage, histological grade, Ki-67 expression, maximum tumor diameter,calcification, and the presence of a coronal skip sign (P<0.05).Multivariate Cox regression analysis identified N3 stage(hazard ratio [HR]=3.762, 95% confidence interval [CI]: 1.147-12.337, P=0.029), histological grade III(HR=3.558, 95%CI: 1.631-7.759, P=0.001), calcification(HR=4.066, 95%CI: 1.888-8.757, P<0.001), and the coronal skip sign(HR=2.178, 95%CI: 1.064-4.460, P=0.033) as independent risk factors for recurrence-free survival in luminal B patients.Three predictive models were developed, with concordance indices (C-index) of 0.687 for the clinicopathological model, 0.734 for the ABUS model, and 0.791 for the combination model.ROC curve analysis demonstrated that the AUC values for the clinicopathological model, ABUS model, and combination model were 0.688, 0.707, and 0.779 in predicting 3-year recurrence risk, and 0.724, 0.745, and 0.819 in predicting 5-year recurrence risk, respectively.The DeLong test indicated that the AUC of the combination model at years was significantly higher than those of the clinicopathological model and the ABUS model (P<0.05).Internal validation revealed satisfactory stability for the combination model (C-index=0.788).The calibration curve of the combination model closely matched the ideal curve.DCA showed that the combination model had higher clinical net benefit within a wide threshold probability range of 3.0% to 81.0%.Survival analysis demonstrated statistically significant differences in cumulative survival rates among patients with varying N stages, histological grades, Ki-67 expression levels, maximum tumor diameters, the presence or absence of calcification, and the presence or absence of a coronal skip sign (P<0.05).
Conclusion
The predictive model established by combining ABUS imaging features with clinicopathological characteristics demonstrates favorable performance, providing an efficient, accurate, and cost-effective approach for predicting postoperative recurrence risk in luminal B breast cancer patients.This model can assist clinicians in assessing recurrence risk and developing individualized followup strategies.
表1 Luminal B 型乳腺癌患者术后未复发组与复发组临床病理及ABUS 图像特征比较[例(%)] |
| 特征 | 总计(n=293) | 未复发(n=257) | 复发(n=36) | 统计值 | P值 |
|---|---|---|---|---|---|
| 年龄[ 岁,M ( Q1, Q3 )] | 47.0(42.0,54.0) | 48.0(42.0,54.5) | 45.5(39.25,51.0) | Z=-1.831 | 0.067 |
| 绝经情况 | χ 2=0. 855 | 0.355 | |||
| 未绝经 | 183(62.5) | 158(61.5) | 25(69.4) | ||
| 已绝经 | 110(37.5) | 99(38.5) | 11(30.6) | ||
| 手术方式 | χ 2=0.568 | 0.494 | |||
| 保乳术后 | 79(27.0) | 71(27.6) | 8(22.2) | ||
| 全切术后 | 214(73.0) | 186(72.4) | 28(77.8) | ||
| 新辅助化疗 | χ 2=1.379 | 0.240 | |||
| 是 | 128(43.7) | 109(42.4) | 19(52.8) | ||
| 否 | 165(56.3) | 148(57.6) | 17(47.2) | ||
| 化疗 | χ 2=0.700 | 0.403 | |||
| 是 | 133(45.4) | 119(46.3) | 14(38.9) | ||
| 否 | 160(54.6) | 138(53.7) | 22(61.1) | ||
| 放疗 | χ 2=0.006 | 0.938 | |||
| 是 | 96(32.8) | 84(32.7) | 12(33.3) | ||
| 否 | 197(67.2) | 173(67.3) | 24(66.7) | ||
| T 分期 | χ 2=4.754 | 0.093 | |||
| 1 | 174(59.4) | 158(61.5) | 16(44.4) | ||
| 2 | 112(38.2) | 94(36.6) | 18(50) | ||
| 3 | 7(2.4) | 5(1.9) | 2(5.6) | ||
| N 分期 | χ 2=9.294 | 0.021 | |||
| 0 | 153(52.2) | 142(55.3) | 11(30.6) | ||
| 1 | 81(27.6) | 68(26.5) | 13(36.1) | ||
| 2 | 43(14.7) | 35(13.6) | 8(22.2) | ||
| 3 | 16(5.5) | 12(4.7) | 4(11.1) | ||
| PR 表达 | χ 2=0.012 | 0.913 | |||
| 阴性 | 39(13.3) | 34(13.2) | 5(13.9) | ||
| 阳性 | 254(86.7) | 223(86.8) | 31(86.1) | ||
| HER2 表达 | χ 2=0.233 | 0.629 | |||
| 阴性 | 100(34.1) | 89(34.6) | 11(30.6) | ||
| 阳性 | 193(65.9) | 168(65.4) | 25(69.4) | ||
| Ki-67 表达 | χ 2=5.794 | 0.016 | |||
| < 30% | 176(60.1) | 161(62.6) | 15(41.7) | ||
| ≥ 30% | 117(39.9) | 96(37.4) | 21(58.3) | ||
| 组织学分级 | χ 2=18.159 | < 0.001 | |||
| Ⅰ / Ⅱ级 | 256(87.4) | 233(90.7) | 23(63.9) | ||
| Ⅲ级 | 37(12.6) | 24(9.3) | 13(36.1) | ||
| 肿瘤最大径 | χ 2=7.683 | 0.021 | |||
| ≤ 2.0 cm | 100(34.1) | 94(36.6) | 6(16.7) | ||
| 2.0 ~ 5.0 cm | 163(55.6) | 140(54.5) | 23(63.9) | ||
| ≥ 5.0 cm | 30(10.2) | 23(8.9) | 7(19.4) | ||
| 形状 | χ 2=3.308 | 0.069 | |||
| 不规则 | 282(96.2) | 249(96.9) | 32(88.9) | ||
| 规则 | 11(3.8) | 8(3.1) | 3(8.3) | ||
| 边缘 | χ 2=0.05 | 0.823 | |||
| 不光整 | 283(96.6) | 248(96.5) | 35(97.2) | ||
| 光整 | 10(3.4) | 9(3.5) | 1(2.8) | ||
| 内部回声 | χ 2=0.05 | 0.823 | |||
| 低回声 | 283(96.6) | 248(96.5) | 35(97.2) | ||
| 混合回声 | 10(3.4) | 9(3.5) | 1(2.8) | ||
| 后方回声 | χ 2=1.862 | 0.394 | |||
| 无改变 | 199(67.9) | 178(69.3) | 21(58.3) | ||
| 增强 | 72(24.6) | 61(23.7) | 11(30.6) | ||
| 衰减 | 22(7.5) | 18(7.0) | 4(11.1) | ||
| 钙化 | χ 2=24.74 | < 0.001 | |||
| 无 | 190(64.8) | 180(70.0) | 10(27.8) | ||
| 有 | 103(35.2) | 77(30.0) | 26(72.2) | ||
| 高回声晕 | χ 2=0.121 | 0.728 | |||
| 无 | 163(55.6) | 142(55.3) | 21(58.3) | ||
| 有 | 130(44.4) | 115(44.7 | 15(41.7) | ||
| 冠状面汇聚征 | χ 2=0.99 | 0.753 | |||
| 无 | 88(30.0) | 78(30.4) | 10(27.8) | ||
| 有 | 205(70.0) | 179(69.6) | 26(72.2) | ||
| 冠状面跳跃征 | χ 2=14.905 | < 0.001 | |||
| 无 | 228(77.8) | 209(81.3) | 19(52.8) | ||
| 有 | 65(22.2) | 48(18.7) | 17(47.2) |
注:ABUS 为自动乳腺超声;PR 为孕激素受体;HER2 为人表皮生长因子受体2 |
表2 Luminal B 型乳腺癌患者术后复发的多因素Cox 回归分析 |
| 因素 | β值 | SE | Wald χ2值 | HR (95% CI ) | P值 |
|---|---|---|---|---|---|
| N 分期 | |||||
| 0 | Ref | ||||
| 1 | 0.597 | 0.417 | 2.047 | 1.817( 0.802 ~ 4.117) | 0.153 |
| 2 | 0.853 | 0.491 | 3.011 | 2.346( 0.895 ~ 6.147) | 0.083 |
| 3 | 1.325 | 0.606 | 4.779 | 3.762( 1.147 ~ 12.337) | 0.029 |
| Ki-67 表达 | |||||
| < 30% | Ref | ||||
| ≥ 30% | 0.490 | 0.368 | 1.772 | 1.632(0.793 ~ 3.358) | 0.183 |
| 组织学分级 | |||||
| Ⅰ / Ⅱ级 | Ref | ||||
| Ⅲ级 | 1.269 | 0.398 | 10.178 | 3.558( 1.631 ~ 7.759) | 0.001 |
| 肿瘤最大径 | |||||
| ≤ 2.0 cm | Ref | ||||
| 2.0 ~ 5.0 cm | 0.263 | 0.479 | 0.302 | 1.301( 0.509 ~ 3.327) | 0.583 |
| ≥ 5.0 cm | 0.299 | 0.616 | 0.236 | 1.349(0.403 ~ 4.509) | 0.627 |
| 钙化 | |||||
| 无 | Ref | ||||
| 有 | 1.403 | 0.391 | 12.835 | 4.066( 1.888 ~ 8.757) | <0.001 |
| 冠状面跳跃征 | |||||
| 无 | Ref | ||||
| 有 | 0.779 | 0.366 | 4.534 | 2.178(1.064 ~ 4.460) | 0.033 |
表3 Luminal B 型乳腺癌术后复发的3 种预测模型效能分析 |
| 模型 | C-index(95%CI) | 准确性(95%CI) | 敏感度(95%CI) | 特异度(95%CI) |
|---|---|---|---|---|
| 临床病理模型 | 0.687(0.593 ~ 0.781) | 0.717(0.669 ~ 0.768) | 0.583(0.425 ~ 0.744) | 0.735(0.683 ~ 0.788) |
| ABUS 模型 | 0.734(0.650 ~ 0.818) | 0.611(0.560 ~ 0.669) | 0.833(0.708 ~ 0.943) | 0.580(0.521 ~ 0.640) |
| 综合模型 | 0.791(0.718 ~ 0.864) | 0.816(0.766 ~ 0.858) | 0.856(0.813 ~ 0.899) | 0.810(0.747 ~ 0.864) |
注:ABUS 为自动乳腺超声;C-index 为一致性指数 |
图4 不同复发风险因素特征的Luminal B 型乳腺癌患者的术后生存曲线。图a 为不同N 分期患者的K-M 生存曲线;图b为不同组织学分级患者的K-M 生存曲线;图c 为Ki-67 高表达与Ki-67 低表达患者的K-M 生存曲线;图d 为不同肿瘤最大径患者的K-M 生存曲线;图e 为存在与不存在钙化患者的K-M 生存曲线;图f 为存在与不存在冠状面跳跃征患者的K-M生存曲线 |
表4 Luminal B 型乳腺癌患者生存分析 |
| 风险因素 | 例数 | 中位生存时间(月) | 累积生存率 | χ 2值 | P值 | |
|---|---|---|---|---|---|---|
| 3 年 | 5 年 | |||||
| N 分期 | 9.013 | 0.029 | ||||
| 0 | 153 | 71.00 | 95% | 94% | ||
| 1 | 81 | 64.00 | 88% | 85% | ||
| 2 | 43 | 67.00 | 91% | 79% | ||
| 3 | 16 | 56.50 | 94% | 77% | ||
| 组织学分级 | 23.713 | < 0.001 | ||||
| Ⅰ / Ⅱ级 | 256 | 70.00 | 94% | 91% | ||
| Ⅲ级 | 37 | 56.00 | 78% | 71% | ||
| Ki-67 | 6.355 | 0.012 | ||||
| 低表达 | 176 | 70.00 | 95% | 92% | ||
| 高表达 | 117 | 65.00 | 89% | 83% | ||
| 肿瘤最大径 | 7.579 | 0.023 | ||||
| ≤ 2.0 cm | 100 | 72.00 | 96% | 93% | ||
| 2.0 ~ 5.0 cm | 163 | 66.00 | 92% | 88% | ||
| ≥ 5.0 cm | 30 | 69.00 | 83% | 76% | ||
| 钙化 | 24.668 | < 0.001 | ||||
| 无 | 190 | 69.50 | 97% | 96% | ||
| 有 | 103 | 65.00 | 84% | 76% | ||
| 冠状面跳跃征 | 13.397 | < 0.001 | ||||
| 无 | 228 | 69.00 | 94% | 92% | ||
| 有 | 65 | 65.00 | 86% | 77% | ||
| 1 |
Bray F, Laversanne M, Sung H, et al.Global cancer statistics 2022:GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J].CA Cancer J Clin, 2024, 74(3): 229-263.
|
| 2 |
Gadaleta E, Thorn GJ, Ross-Adams H, et al.Field cancerization in breast cancer[J].J Pathol, 2022, 257(4): 561-574.
|
| 3 |
国家肿瘤质控中心乳腺癌专家委员会, 北京乳腺病防治学会健康管理专业委员会.中国乳腺癌随诊随访与健康管理指南(2022版)[J].中华肿瘤杂志, 2022(1): 1-28.
|
| 4 |
Metzger-Filho O, Sun Z, Viale G, et al.Patterns of recurrence and outcome according to breast cancer subtypes in lymph node-negative disease: results from international breast cancer study group trials VIII and IX[J].J Clin Oncol, 2013, 31(25): 3083-3090.
|
| 5 |
Ignatiadis M, Bedard P, Haibe-Kains B, et al.A meta-analysis of gene expression profiling studies identifies clinically relevant oncogenic pathways in basal-like breast cancer[J].Cancer Research, 2009,69(24_Supplement): 106.
|
| 6 |
Tran B, Bedard PL.Luminal-B breast cancer and novel therapeutic targets[J].Breast Cancer Research, 2011, 13(6): 221.
|
| 7 |
中国抗癌协会乳腺癌专业委员会, 中华医学会肿瘤学分会乳腺肿瘤学组.中国抗癌协会乳腺癌诊治指南与规范(2024 年版)[J].中国癌症杂志, 2023, 33(12): 1092-1187.
|
| 8 |
Sparano JA, Gray RJ, Ravdin PM, et al.Clinical and genomic risk to guide the use of adjuvant therapy for breast cancer[J].N Engl J Med,2019, 380(25): 2395-2405.
|
| 9 |
Dang X, Gao Y, Ju Y, et al.Automated breast ultrasound with remote reading for primary breast cancer screening: a prospective study involving 46 community health centers in China[J].AJR Am J Roentgenol, 2025, 224(1): e2431830.
|
| 10 |
中国超声医学工程学会仪器工程开发专业委员会, 中国抗癌协会肿瘤影像专委会, 中华医学会超声医学分会浅表组织与血管学组.自动乳腺容积超声技术专家共识(2022 版)[J].中国超声医学杂志,2022, 38(3): 241-247.
|
| 11 |
Vourtsis A, Kachulis A.The performance of 3D ABUS versus HHUS in the visualisation and BI-RADS characterisation of breast lesions in a large cohort of 1,886 women[J].Eur Radiol, 2018, 28(2): 592-601.
|
| 12 |
Gradishar WJ, Moran MS, Abraham J, et al.Breast Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology[J].J Natl Compr Canc Netw, 2024, 22(5): 331-357.
|
| 13 |
Edge Sb BD, Compton Cc, Fritz Ag, et al.AJCC cancer staging manual [M].7th ed.NY: Springer, 2010.
|
| 14 |
Böcker W.[WHO classification of breast tumors and tumors of the female genital organs: pathology and genetics][J].Verh Dtsch Ges Pathol, 2002, 86: 116-119.
|
| 15 |
Mendelson EB, Böhm-Vélez M, Berg WA, et al.ACR BI-RADS Ultrasound.ACR BI-RADS Atlas, Breast Imaging Reporting and Data System[S].Reston: American College of Radiology, 2013.
|
| 16 |
Hanahan D, Weinberg RA.Hallmarks of cancer: the next generation[J].Cell, 2011, 144(5): 646-674.
|
| 17 |
Ades F, Zardavas D, Bozovic-Spasojevic I, et al.Luminal B breast cancer: molecular characterization, clinical management, and future perspectives[J].J Clin Oncol, 2014, 32(25): 2794-2803.
|
| 18 |
Lyngholm CD, Laurberg T, Alsner J, et al.Failure pattern and survival after breast conserving therapy.Long-term results of the Danish Breast Cancer Group (DBCG) 89 TM cohort[J].Acta Oncol, 2016, 55(8):983-992.
|
| 19 |
Yu NY, Iftimi A, Yau C, et al.Assessment of long-term distant recurrence-free survival associated with Tamoxifen therapy in postmenopausal patients with Luminal A or Luminal B breast cancer[J].JAMA Oncol, 2019, 5(9): 1304-1309.
|
| 20 |
Pan H, Gray R, Braybrooke J, et al.20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years[J].N Engl J Med, 2017, 377(19): 1836-1846.
|
| 21 |
Braunstein LZ, Taghian AG, Niemierko A, et al.Breast-cancer subtype, age, and lymph node status as predictors of local recurrence following breast-conserving therapy[J].Breast Cancer Res Treat, 2017,161(1): 173-179.
|
| 22 |
Rakha EA, Reis-Filho JS, Baehner F, et al.Breast cancer prognostic classification in the molecular era: the role of histological grade[J].Breast Cancer Research, 2010, 12(4): 207.
|
| 23 |
Saadatmand S, Bretveld R, Siesling S, et al.Influence of tumour stage at breast cancer detection on survival in modern times: population based study in 173,797 patients[J].BMJ, 2015, 351: h4901.
|
| 24 |
Davey MG, Hynes SO, Kerin MJ, et al.Ki-67 as a prognostic biomarker in invasive breast cancer[J].Cancers (Basel), 2021, 13(17):4455.
|
| 25 |
Zheng K, Tan J-X, Li F, et al.Relationship between mammographic calcifications and the clinicopathologic characteristics of breast cancer in Western China: a retrospective multi-center study of 7317 female patients[J].Breast Cancer Res Treat, 2017, 166(2): 569-582.
|
| 26 |
Li Y, Cao J, Zhou Y, et al.Mammographic casting-type calcification is an independent prognostic factor in invasive breast cancer[J].Sci Rep,2019, 9(1): 10544.
|
| 27 |
Qi X, Chen A, Zhang P, et al.Mammographic calcification can predict outcome in women with breast cancer treated with breast-conserving surgery[J].Oncol Lett, 2017, 14(1): 79-88.
|
| 28 |
Van Zelst JCM, Mann RM.Automated three-dimensional breast US for screening: technique, artifacts, and lesion characterization[J].Radiographics, 2018, 38(3): 663-683.
|
| 29 |
Zheng FY, Lu Q, Huang BJ, et al.Imaging features of automated breast volume scanner: Correlation with molecular subtypes of breast cancer[J].Eur J Radiol, 2017, 86: 267-275.
|
| 30 |
Karst I, Henley C, Gottschalk N, et al.Three-dimensional automated breast US: facts and artifacts[J].Radiographics, 2019, 39(4): 913-931.
|
| 31 |
Kim SH.Image quality and artifacts in automated breast ultrasonography[J].Ultrasonography, 2019, 38(1): 83-91.
|
| 32 |
Safaei S, Sajed R, Shariftabrizi A, et al.Tumor matrix stiffness provides fertile soil for cancer stem cells[J].Cancer Cell Int, 2023,23(1): 143.
|
| 33 |
Mao N, Yin P, Zhang H, et al.Mammography-based radiomics for predicting the risk of breast cancer recurrence: a multicenter study[J].Br J Radiol, 2021, 94(1127): 20210348.
|
| 34 |
闫静茹, 高喜璨, 巨艳, 等.自动乳腺容积超声成像与乳腺X 线、常规手持超声检查患者接受度的对比分析研究[J].中华超声影像学杂志, 2017, 26(9): 787-792.
|
| 35 |
Xu K, Hua M, Mai T, et al.A multiparametric MRI-based radiomics model for stratifying postoperative recurrence in Luminal B breast cancer[J].J Imaging Inform Med, 2024, 37(4): 1475-1487.
|
| 36 |
Xiong L, Chen H, Tang X, et al.Ultrasound-based radiomics analysis for predicting disease-free survival of invasive breast cancer[J].Front Oncol, 2021, 11: 621993.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}