
2025 , Vol. 22 >Issue 09: 858 - 867
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.09.011
甲状腺乳头状癌术后颈部转移淋巴结超声引导下微波消融与再次手术的疗效比较
通信作者:
曾锦树,Email:zengjinshu761129@163.comCopy editor: 吴春凤
收稿日期: 2025-07-02
网络出版日期: 2025-12-24
版权
Efficacy of ultrasound-guided microwave ablation versus reoperation for cervical metastatic lymph nodes in patients after surgery for papillary thyroid cancer
Corresponding author:
Zeng Jinshu, Email: zengjinshu761129@163.comReceived date: 2025-07-02
Online published: 2025-12-24
Copyright
探讨与传统再次手术相比,超声引导下经皮微波消融治疗甲状腺乳头状癌(PTC)术后复发性颈部转移淋巴结的效果、安全性及经济性,为临床提供参考。
回顾性分析2021年12月至2023年12月福建医科大学附属第一医院收治的53例PTC术后复发性颈部转移淋巴结患者,根据治疗方式分为微波消融组(15例)和再次手术组(38例)。采用倾向性评分结合逆概率加权(IPTW)方法控制组间基线差异,微波消融组术后1、3、6、12个月的病灶最大直径、体积、体积缩小率(VRR)及血清Tg水平差异采用重复测量资料方差分析;加权后组间差异比较采用加权t检验、加权秩检验、Rao-Scott校正χ2检验,组内差异比较采用配对t检验、Wilcoxon符号秩检验,比较2组手术相关指标(住院时间、手术时间、术中出血量、切口长度、住院费用)及术前和术后1个月的甲状腺功能、血清甲状腺球蛋白(Tg)水平的变化,且进一步对术前血清Tg≥1 ng/ml的患者进行亚组分析。
IPTW后,微波消融组住院时间、手术时间、术中出血量、切口长度、住院费用均低于再次手术组[(1.00±0.01)d vs(7.44±1.37)d;0.3(0.3,0.3)h vs 2.1(1.5,2.8)h;1.0(1.0,1.0)ml vs 10.0(5.0,10.0)ml;0.2(0.1,0.2)cm vs 6.0(6.0,12.0)cm;2699.3(2285.7,8318.4)元 vs 15 293.5(11 263.5,18 655.7)元],差异具有统计学意义(t=28.18、Z=4.86、Z=6.84、Z=6.37、Z=4.36,P均<0.001)。微波消融组19枚淋巴结均成功消融,治疗后病灶最大直径、体积、VRR及血清Tg水平均明显下降,差异具有统计学意义(P均<0.05)。再次手术组术后1个月血清Tg变化与术前及微波消融组比较均降低[0.66(0.16,5.84)ng/ml vs 2.22(0.86,11.11)ng/ml vs 5.50(1.00,8.00)ng/ml],差异具有统计学意义(Z=-2.589、-4.404,P=0.010、<0.001),再次手术组术前血清Tg≥1 ng/ml患者的Tg转阴率(46.4%)数值上高于微波消融组(41.7%),但差异未达统计学意义(P>0.05)。并发症方面,2组均无严重并发症,差异无统计学意义(P>0.05),随访期内仅再次手术组出现1例复发。
超声引导下微波消融治疗PTC术后复发性颈部转移淋巴结具有微创、安全、恢复快、费用低等优势,或可作为某些不适合或不愿意接受二次手术患者的替代方案之一。
高昕雨 , 杨楷熠 , 陈慧婷 , 朱丽 , 方雅滨 , 宋梅 , 曾锦树 . 甲状腺乳头状癌术后颈部转移淋巴结超声引导下微波消融与再次手术的疗效比较[J]. 中华医学超声杂志(电子版), 2025 , 22(09) : 858 -867 . DOI: 10.3877/cma.j.issn.1672-6448.2025.09.011
To compare the effectiveness, safety, and cost of ultrasound-guided percutaneous microwave ablation versus conventional reoperation for cervical metastatic lymph nodes in patients after surgery for papillary thyroid carcinoma and to provide reference for clinical practice.
This retrospective study included 53 patients with postoperative cervical metastatic lymph nodes treated at the First Affiliated Hospital of Fujian Medical University from December 2021 to December 2023, who were assigned to either a microwave ablation group (15 cases) or a reoperation group (38 cases) according to the treatment modality used. Baseline differences were controlled using propensity scoring combined with inverse probability of treatment weighting (IPTW). In the microwave ablation group, the maximum lesion diameter, lesion volume, volume reduction ratio (VRR), and serum thyroglobulin levels at 1, 3, 6, and 12 months after treatment were analyzed by repeated-measures analysis of variance. Between-group comparisons after weighting were performed using weighted t tests, weighted rank-sum tests, and the Rao-Scott corrected chi-square test, while within-group comparisons were conducted using paired t tests and the Wilcoxon signed-rank test. Surgical indicators (length of stay, operative time, intraoperative blood loss, incision length, and hospitalization costs), as well as thyroid function and serum thyroglobulin pre-treatment and 1 month post-treatment were compared. A subgroup analysis was performed among patients with baseline serum thyroglobulin ≥1 ng/ml.
After IPTW, the microwave ablation group showed significantly shorter length of stay and operative time as well as lower intraoperative blood loss, incision length, and hospitalization costs than the reoperation group [(1.00±0.01) d vs (7.44±1.37) d, 0.3(0.3, 0.3) h vs 2.1(1.5, 2.8) h, 1.0 (1.0, 1.0) ml vs 10.0 (5.0, 10.0) ml, 0.2 (0.1, 0.2) cm vs 6.0 (6.0, 12.0) cm, and 2699.3 (2285.7, 8318.4) yuan vs 15293.5 (11263.5, 18655.7) yuan, respectively; t=28.18; Z=4.86, 6.84, 6.37, and 4.36, respectively; all P<0.001). All 19 lymph nodes in the microwave ablation group were successfully ablated. Post-treatment, the mean maximum lesion diameter, lesion volume, volume reduction ratio, VRR, and serum thyroglobulin decreased significantly over time (all P<0.05). At 1 month post-treatment, changes in serum thyroglobulin in the reoperation group were statistically different from pretreatment and from the microwave ablation group (0.66 (0.16, 5.84) ng/ml vs 2.22 (0.86, 11.11) ng/ml vs 5.50 (1.00, 8.00) ng/ml; Z=−2.589 and −4.404; P=0.010 and <0.001, respectively). The thyroglobulin negativity rate was numerically higher in the reoperation group (46.4%) than in the microwave ablation group (41.7%), but the difference was not significant (P>0.05). No severe complications occurred in either group, with no significant between-group difference (P>0.05). During follow-up, only one case of recurrence occurred, in the reoperation group.
Ultrasound-guided percutaneous microwave ablation for cervical metastatic lymph nodes recurring after surgery for papillary thyroid carcinoma offers the advantages of minimal invasiveness, safety, rapid recovery, and lower costs, and may serve as an alternative for patients who are unsuitable for or unwilling to undergo a second operation.

表1 甲状腺乳头状癌术后复发性颈部转移淋巴结患者IPTW前后的基线资料比较 |
| 变量 | IPTW前 | IPTW后 | ||||||
|---|---|---|---|---|---|---|---|---|
| 再次手术组(38例) | 微波消融组(15例) | P值 | SMD值 | 再次手术组(38例) | 微波消融组(15例) | P值 | SMD值 | |
年龄(岁, | 45.28±13.59 | 46.79±13.51 | 0.202 | 0.39 | 45.35±13.66 | 43.83±11.45 | 0.679 | 0.12 |
| 性别[例(%)] | 0.665 | 0.23 | 0.724 | 0.13 | ||||
| 男 | 16(42.1) | 8(53.3) | 15.1(39.7) | 5.0(33.7) | ||||
| 女 | 22(57.9) | 7(46.7) | 22.9(60.3) | 10.0(66.3) | ||||
最大径(cm, | 1.05±0.26 | 1.14±0.32 | 0.313 | 0.29 | 1.06±0.26 | 1.05±0.29 | 0.911 | 0.04 |
随访时间(月, | 15.84±4.76 | 19.73±6.90 | 0.023 | 0.66 | 16.92±5.50 | 17.06±5.49 | 0.939 | 0.03 |
| 术前是否接受碘剂治疗[例(%)] | 0.092 | 0.66 | 0.932 | 0.04 | ||||
| 否 | 19(50.0) | 3(20.0) | 22.2(58.4) | 9.3(62.0) | ||||
| 是 | 19(50.0) | 12(80.0) | 15.8(41.6) | 5.7(38.0) | ||||
| 共病指数[例(%)] | 0.494 | 0.36 | 0.963 | 0.09 | ||||
| 0种 | 29(76.3) | 9(60.0) | 28.0(73.6) | 10.7(71.3) | ||||
| 1种 | 6(15.8) | 4(26.7) | 6.4(16.7) | 2.4(16.3) | ||||
| 2种 | 3(7.9) | 2(13.3) | 3.7(9.7) | 1.9(12.4) | ||||
| 淋巴结位置[例(%)] | 0.403 | 0.39 | 0.554 | 0.22 | ||||
| 中央区 | 11(28.9) | 2(13.3) | 9.2(24.2) | 2.4(16.0) | ||||
| 侧颈区 | 27(71.1) | 13(86.7) | 28.8(75.8) | 12.6(84.0) | ||||
注:IPTW为逆概率加权法,SMD为标准化均数差;a以患者为基础的分析:无论患者有无侧颈区淋巴结转移,若中央区出现颈部转移性淋巴结则视为中央区淋巴结转移 |
表2 甲状腺乳头状癌术后复发性颈部转移淋巴结患者不同治疗方式组手术相关指标比较 |
| 变量 | IPTW前 | |||
| 微波消融组(15例) | 再次手术组(38例) | 统计值 | P值 | |
| 住院时间[d,M(Q1,Q3)] | 1.0(1.0,1.0) | 7.0(6.0,8.0) | U=0.50 | <0.001 |
手术时间(h, | 0.33±0.08 | 2.12±0.83 | t=13.13 | <0.001 |
| 术中出血量[ml,M(Q1,Q3)] | 1.0(0.5,1.0) | 10.0(5.0,10.8) | U=0.00 | <0.001 |
| 切口长度[cm,M(Q1,Q3)] | 0.2(0.1,0.2) | 6.0(6.0,12.0) | U=0.00 | <0.001 |
| 住院费用[元,M(Q1,Q3)] | 3523.4(2300.2,10 314.7) | 15 489.9(11 635.4,18 683.4) | U=39.00 | <0.001 |
| 并发症[例(%)] | 3(20.0) | 7(18.4) | χ2=0.02 | 0.895 |
| 生存率[例(%)] | 15(100) | 38(100) | ||
| 变量 | IPTW后 | |||
| 微波消融组(15例) | 再次手术组(38例) | 统计值 | P值 | |
住院时间(d, | 1.00±0.01 | 7.44±1.37 | t=28.18 | <0.001 |
| 手术时间[h,M(Q1,Q3)] | 0.3(0.3,0.3) | 2.1(1.5,2.8) | Z=4.86 | <0.001 |
| 术中出血量[ml,M(Q1,Q3)] | 1.0(1.0,1.0) | 10.0(5.0,10.0) | Z=6.84 | <0.001 |
| 切口长度[cm,M(Q1,Q3)] | 0.2(0.1,0.2) | 6.0(6.0,12.0) | Z=6.37 | <0.001 |
| 住院费用[元,M(Q1,Q3)] | 2699.3(2285.7,8318.4) | 15 293.5(11 263.5,18 655.7) | Z=4.36 | <0.001 |
| 并发症[例(%)] | 3(20.0) | 5(13.2) | χ2=0.55 | 0.525 |
| 生存率[例(%)] | 15(100) | 38(100) | ||
注:IPTW为逆概率加权法,生存率比例一致,检验无区分力,仅作描述 |
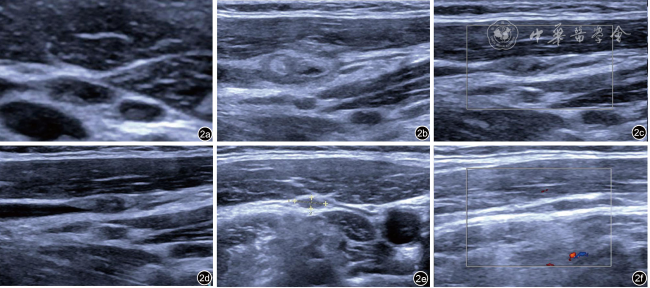
图2 甲状腺乳头状癌复发性颈部转移性淋巴结消融术前、术后超声图像。图a为术前颈部转移性淋巴结;图b为消融术后1个月复查图,可见混合不均匀回声区,以高回声为主,范围较原有淋巴结稍大;图c为术后3个月复查图,可见混合不均匀稍高回声区较前次复查缩小;图d为术后6个月复查图,与前次复查相仿;图e为术后12个月复查图,稍高回声区较前次复查缩小;图f为术后18个月复查图,原稍高回声区几乎显示不清,考虑消融灶几乎完全吸收 |
表3 甲状腺乳头状癌术后复发性颈部转移淋巴结超声引导下微波消融术前后相关指标变化 |
| 时间 | 最大直径(cm, | 体积(cm3, | VRR(%, | Tg[ng/ml,M(Q1,Q3)] |
|---|---|---|---|---|
| 微波消融术前 | 1.14±0.32 | 0.19±0.12 | 0.00±0.00 | 9.37(3.59,17.22) |
| 微波消融后1个月 | 0.96±0.36 | 0.15±0.13 | 20.82±26.86 | 6.10(1.00,12.00) |
| 微波消融后3个月 | 0.83±0.33 | 0.07±0.06 | 67.21±23.82 | 1.91(0.78,4.00) |
| 微波消融后6个月 | 0.72±0.33 | 0.02±0.02 | 87.70±14.24 | 0.40(0.04,1.38) |
| 微波消融后12个月 | 0.60±0.31 | 0.02±0.02 | 91.83±10.16 | 0.06(0.03,1.06) |
| F值 | 20.892 | 23.205 | 87.885 | 18.262 |
| P值 | <0.001 | <0.001 | <0.001 | <0.001 |
注:VRR为体积缩小率,Tg为甲状腺球蛋白;*Tg数据呈偏态分布,做ln(Tg+0.1)变换后进行分析;a与微波消融术前比较,差异具有统计学意义(最大直径:q=3.894,P=0.008;q=6.828,P<0.001;q=9.196,P<0.001;q=11.724,P<0.001;体积:q=7.638,P<0.001;q=10.570,P<0.001;q=10.776,P<0.001;VRR:q=4.788,P=0.001;q=15.338,P<0.001;q=20.020,P<0.001;q=20.962,P<0.001;Tg:q=6.702,P<0.001;q=8.352,P<0.001;q=10.215,P<0.001)。以上数据均采用原始数据分析所得 |
表4 甲状腺乳头状癌术后复发性颈部转移淋巴结患者不同治疗方式组甲状腺激素水平比较[M(Q1,Q3)/ |
| 组别 | 例数 | TSH(ml/UL) | FT3(pmol/L) | FT4(pmol/L) | Tg(ng/ml) |
| 微波消融组 | 15 | ||||
| 术前 | 1.65(0.30,7.28) | 4.84±0.63 | 20.10±2.73 | 9.90(2.88,15.50) | |
| 术后1个月 | 0.09(0.05,1.06) | 4.65±0.81 | 20.55±2.58 | 5.50(1.00,8.00) | |
| 统计值 | Z=-1.882 | t=-0.795 | t=-0.421 | Z=-1.489 | |
| P值 | 0.064 | 0.442 | 0.681 | 0.136 | |
| 再次手术组 | 38 | ||||
| 术前 | 0.60(0.12,2.18) | 5.02(4.63,5.99) | 18.90(17.33,22.10) | 2.22(0.86,11.11) | |
| 术后1个月 | 0.63(0.15,4.10) | 4.60(4.00,5.65) | 19.50(18.88,22.62) | 0.66(0.16,5.84) | |
| Z值 | -0.907 | -1.775 | -0.613 | -2.589 | |
| P值 | 0.364 | 0.076 | 0.540 | 0.010 | |
| Z值 | 1.315 | -0.203 | -1.391 | -1.691 | |
| P值 | 0.190 | 0.839 | 0.164 | 0.091 | |
| Z值 | -0.660 | -1.407 | -0.026 | -4.404 | |
| P | 0.509 | 0.160 | 0.979 | <0.001 |
注:TSH为促甲状腺激素,FT3为游离三碘甲状腺原氨酸,FT4为游离甲状腺素,Tg为甲状腺球蛋白;a为2组间术前各指标差异比较的结果,b为2组间术后1个月各指标差异比较的结果;以上结果均为原始数据经逆概率加权法处理后再分析所得 |
表5 甲状腺乳头状癌术后复发性颈部转移淋巴结不同治疗方式组中血清Tg≥1 ng/ml患者的Tg变化比较 |
| 项目 | 微波消融组(15例) | 再次手术组(38例) | 统计值 | P值 |
|---|---|---|---|---|
| 术前 | ||||
| Tg≥1 ng/ml患者[例(%)] | 12(80.0) | 28(73.7) | χ2=1.566 | 0.211 |
| Tg水平[ng/ml,M(Q1,Q3)] | 10.50(3.72,15.60) | 5.46(2.22,15.80) | Z=-0.295 | 0.768 |
| 术后 | ||||
| Tg≥1 ng/ml患者[例(%)] | 7(46.7) | 15(39.5) | χ2=0.213 | 0.644 |
| Tg水平[ng/ml,M(Q1,Q3)] | 8.00(6.46,11.15) | 6.01(5.63,7.92) | Z=1.271 | 0.203 |
| Tg下降值[ng/ml,M(Q1,Q3)] | 2.92(0.99,10.57) | 2.04(0.83,11.75) | Z=0.811 | 0.417 |
| Tg转阴患者[例(%)] | 5(41.7) | 13(46.4) | χ2=0.021 | 0.885 |
注:Tg为甲状腺球蛋白;a术前血清Tg≥1 ng/ml的患者为基数;以上结果均为原始数据经逆概率加权法处理后再分析所得 |
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
|
| 8 |
|
| 9 |
|
| 10 |
葛明华, 徐栋, 杨安奎, 等. 甲状腺良性结节、微小癌及颈部转移性淋巴结热消融治疗专家共识(2018版) [J]. 中国肿瘤, 2018, 27(10): 768-773.
|
| 11 |
|
| 12 |
徐震纲, 刘绍严. 分化型甲状腺癌颈侧区淋巴结清扫专家共识(2017版) [J]. 中国实用外科杂志, 2017, 37(9): 985-991.
|
| 13 |
闫肖, 喻庆安, 高旭, 等. 甲状腺球蛋白在评估分化型甲状腺癌淋巴结转移中的研究进展 [J]. 中国普外基础与临床杂志, 2022, 29(1): 124-129.
|
| 14 |
|
| 15 |
National Health Commission Of The People's Republic Of China. National guidelines for diagnosis and treatment of thyroid cancer 2022 in China (English version) [J]. Chin J Cancer Res, 2022, 34(3): 131-150.
|
| 16 |
|
| 17 |
|
| 18 |
|
| 19 |
付强, 李威, 满文玲, 等. 微波消融治疗甲状腺乳头状癌术后淋巴结转移的临床研究和疗效观察 [J]. 实用肿瘤学杂志, 2020, 34(5): 436-439.
|
| 20 |
|
| 21 |
陈杭军, 张超, 黄品同. 甲状腺微小乳头状癌经微波消融与手术切除的疗效、安全性及经济性比较 [J/CD]. 中华医学超声杂志(电子版), 2018, 15(4): 275-280.
|
| 22 |
|
| 23 |
|
| 24 |
|
| 25 |
|
| 26 |
|
| 27 |
|
| 28 |
|
| 29 |
徐菁菁, 何年安, 叶显俊, 等. 经皮喉超声在评估甲状腺微波消融术患者喉返神经功能变化中的应用[J/OL]. 中华医学超声杂志(电子版), 2025, 22(3): 224-229.
|
| 30 |
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}