
先天性心脏病(congenital heart disease,CHD)是引起儿童死亡的主要原因[1],法洛四联症(tetralogy of Fallot,TOF)占所有CHD的3%~5%[2]。产前准确诊断TOF可积极采取干预措施,避免新生儿早期发绀,提高患儿远期存活率[3]。最近,胎儿心脏超声智能导航技术(FINE或5D Heart)及虚拟智能超声辅助技术(VIS-Assistance®)的发展,进一步简化了胎儿超声心动图的操作,提高了诊断切面的显示率[4, 5, 6]。Yeo等[7, 8]将FINE应用于TOF伴肺动脉闭锁胎儿,但研究为个案报道。目前,关于FINE在胎儿TOF诊断中的应用价值的较大样本、系统性研究报道鲜见。本研究旨在探讨5D Heart技术联合VIS-Assistance®技术在最常见的胎儿经典型TOF诊断中的应用价值。
资料与方法
一、对象
在2015年2月至2020年1月于浙江大学医学院附属邵逸夫医院接受胎儿超声心动图检查的孕妇中选取研究对象进行前瞻性研究。纳入标准:(1)经二维胎儿超声心动图诊断为经典型TOF胎儿的中晚孕期孕妇;(2)单胎妊娠,胎儿脊柱位于2至10点钟位置;(3)根据产科超声(胎儿的双顶径和股骨长)计算的孕龄与停经史计算的孕龄相符(相差≤2周)。排除标准:(1)孕妇腹壁脂肪厚;(2)胎儿频繁运动;(3)羊水过少;(4)TOF合并肺动脉闭锁或肺动脉瓣缺如。满足上述任何1项排除标准,则不纳入研究。
初步入选的60例孕妇中3例由于容积数据无法成功获取而剔除,最终纳入57例胎儿。孕妇年龄20~41(31.0±4.9)岁,孕龄18~36(25.0±3.3)周。所有研究对象在检查前均被充分告知胎儿超声心动图的准确性及局限性,均签署知情同意书。本研究已获得浙江大学医学院附属邵逸夫医院伦理委员会的批准(批准号为20170105-10)。
二、仪器与方法
1.仪器:应用三星WS80A彩色多普勒超声诊断仪,CV1-8探头,频率为1~8 MHZ,配备胎儿心脏超声检查及分析功能。
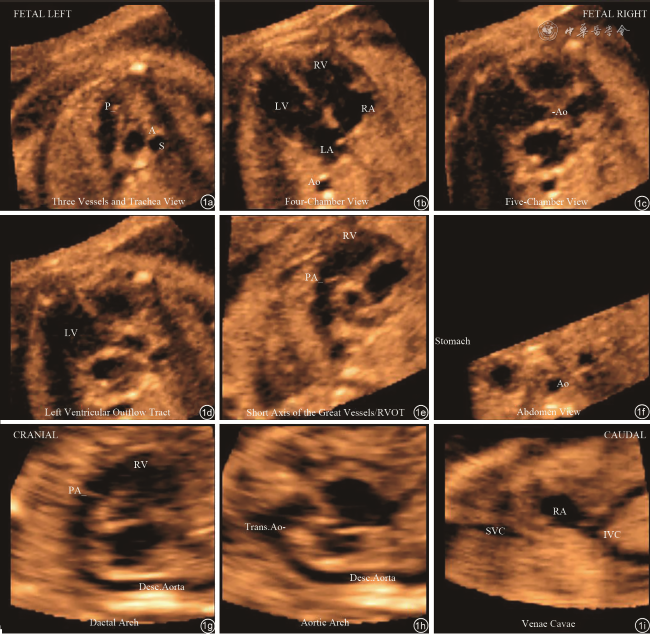
图1 应用5D Heart联合 VIS-Assistance®技术显示孕23周正常胎儿心脏的9个诊断切面。图a为三血管气管切面;图b为四腔心切面;图c为五腔心切面;图d为左心室流出道切面;图e为右心室流出道切面;图f为胃泡水平腹部横切面;图g为动脉导管弓切面;图h为主动脉弓切面;图i为上下腔静脉右心房切面 |

4.评价方法:根据胎儿经典型TOF解剖特点[11]及国际妇产超声协会(ISUOG)在2013年发布的胎儿心脏超声筛查实践指南[12],分别对TOF的5个诊断切面以及17个主要诊断要素进行评分。5个诊断切面分别为:三血管气管切面(3VT)、四腔心切面(4CV)、左心室流出道切面(LVOT)、右心室流出道切面(RVOT)、胃泡切面(Abdomen/Stomach)。17个诊断要素分别为:3VT中扩张的主动脉、狭窄的肺动脉主干、气管、上腔静脉;4CV中4个房室腔、房室瓣、房室瓣距离、卵圆孔瓣、十字交叉、室间隔、调节束;LVOT中室间隔缺损、扩张的主动脉、主动脉骑跨;RVOT中狭窄的肺动脉主干;Abdomen/Stomach中胃泡、降主动脉。各诊断要素根据图像质量进行评分,评分标准分为3个等级[13]:结构清晰,评3分(优);结构不够清晰但可以辨认,评2分(一般);结构模糊不能辨认,评1分(差)。每个诊断切面中的各个诊断要素评分均≥2分,则认为该诊断平面显示成功;若该诊断平面内有1个或1个以上的诊断要素被评为1分,则视为该诊断平面显示失败。每个诊断切面内各个诊断要素总分除以要素个数,即为该诊断平面得分。
5.重复性及一致性检测:应用5D Heart联合VIS-Assistance®技术,医师B及C独立对最优容积数据的各诊断切面及诊断要素进行评分;间隔1个月后,2位医师用同样的方法再一次复评。
6.TOF的诊断:由新生儿超声心动图检查或手术或者尸检等证实TOF的最终诊断,如因各种原因无此类信息,则根据专家进行的胎儿超声心动图结果作为最终诊断[4]。
三、数据记录及分组
依据医师B记录的脊柱位置分为3个亚组:亚组A(脊柱2~4点钟)、亚组B(脊柱5~7点钟)、亚组C(脊柱8~10点钟)。
四、统计学分析
本研究样本量选择是通过R语言(版本:4.0.4)中的pwr包来计算的,根据实验设计要求,将无效假设定为0.25,power是0.95,显著水平=0.05时,经过卡方检验计算得出总样本量至少为39例,当power=0.90而其他条件不变时,总样本量只需要31例,分组的最小样本量不受影响。因此本研究中的57例样本量已经达到了最小样本量的要求。本研究采用SAS 9.4软件对资料进行统计分析,孕龄与年龄以
±s表示,评分以M(P25,P75)表示,两组间的比较采用非参数秩和检验;各诊断切面及诊断要素显示率以例(%)表示,多组间的比较采用χ2检验;以P<0.05为差异具有统计学意义。

{kind=link}
{kind=link}
{kind=link}
{kind=link}
结果
一、TOF胎儿分组
根据脊柱位置将57例TOF胎儿分为3个亚组:亚组A 18例(31.6%),亚组B 28例(49.1%),亚组C 11例(19.3%)。
二、各亚组诊断切面的显示率
根据医师B第一次评分结果,亚组A、B、C中5个诊断切面的显示率分别为66.7%~100.0%、75.0%~100.0%和81.8%~100.0%,不同脊柱位置的5个诊断切面显示率差异均无统计学意义(均P>0.05,表1 )。
表1 不同亚组法洛四联症患儿5D Heart联合VIS-Assistance®技术对各诊断切面的显示率[例(%)] |
| 切面 | 合计(n=57) | 亚组A(n=18) | 亚组B(n=28) | 亚组C(n=11) | χ2值 | P值 |
|---|---|---|---|---|---|---|
| 3VT | 45(78.9) | 12(66.7) | 24(85.7) | 9(81.8) | 2.459 | 0.292 |
| 4CV | 44(77.2) | 12(66.7) | 21(75.0) | 11(100.0) | 4.459 | 0.108 |
| LVOT | 55(96.5) | 18(100.0) | 26(92.9) | 11(100.0) | 2.147 | 0.342 |
| RVOT | 51(89.5) | 16(88.9) | 25(89.3) | 10(90.9) | 0.032 | 0.984 |
| Abdomen/Stomach | 57(100.0) | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
注:3VT为三血管气管切面;4CV为四腔心切面;LVOT为左心室流出道切面;RVOT为右心室流出道切面;Abdomen/Stomach为胃泡切面;-为无数据 |
三、各亚组诊断要素的显示率
根据医师B第一次评分结果,亚组A、B、C中17个主要诊断要素的显示率分别为66.7%~100.0%、78.6%~100.0%和81.8%~100.0%,不同脊柱位置的17个诊断要素显示率差异均无统计学意义(均P>0.05,表2 )。
表2 不同亚组法洛四联症患儿5D Heart联合VIS-Assistance®技术对各诊断要素的显示率[例(%)] |
| 诊断要素 | 亚组A(n=18) | 亚组B(n=28) | 亚组C(n=11) | χ2值 | P值 |
|---|---|---|---|---|---|
| 3VT | |||||
扩张的主动脉 | 16(88.9) | 28(100.0) | 11(100.0) | 4.491 | 0.106 |
狭窄的肺动脉主干 | 17(94.4) | 27(96.4) | 10(90.9) | 0.487 | 0.784 |
气管 | 13(72.2) | 26(92.9) | 9(81.8) | 3.567 | 0.168 |
上腔静脉 | 16(88.9) | 26(92.9) | 10(90.9) | 0.217 | 0.897 |
| 4CV | |||||
4个房室腔 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
房室瓣 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
房室瓣距离 | 17(94.4) | 25(89.3) | 11(100.0) | 1.476 | 0.478 |
卵圆孔瓣 | 12(66.7) | 22(78.6) | 11(100.0) | 4.569 | 0.102 |
十字交叉 | 18(100.0) | 25(89.3) | 11(100.0) | 3.280 | 0.194 |
室间隔 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
调节束 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
| LVOT | |||||
室间隔缺损 | 18(100.0) | 26(92.9) | 11(100.0) | 2.147 | 0.342 |
扩张的主动脉 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
主动脉骑跨 | 18(100.0) | 26(92.9) | 11(100.0) | 2.147 | 0.342 |
| RVOT | |||||
狭窄的肺动脉主干 | 16(88.9) | 25(89.3) | 10(90.9) | 0.032 | 0.984 |
| Abdomen/Stomach | |||||
胃泡 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
降主动脉 | 18(100.0) | 28(100.0) | 11(100.0) | - | - |
注:3VT为三血管气管切面;4CV为四腔心切面;LVOT为左心室流出道切面;RVOT为右心室流出道切面;Abdomen/Stomach为胃泡切面;-为无数据 |
四、不同年资的2位医师各诊断要素的显示率
医师B和医师C分别两次评价诊断要素的显示率如下:3VT中,扩张的主动脉、狭窄的肺动脉主干、上腔静脉的显示率分别为94.7%~96.5%、93.0%~98.2%和86.0%~91.2%。医师B两次评价气管的显示率分别为84.2%、82.5%。医师C 两次评价气管的显示率分别为70.2%、70.2%。4CV中,4个房室腔、房室瓣、室间隔及调节束的显示率均为100.0%。房室瓣距离、卵圆孔瓣和十字交叉的显示率分别为93.0%~96.5%、78.9%~82.5%和94.7%~96.5%。LVOT中,扩张的主动脉显示率均为100.0%,室间隔缺损的显示率为96.5%~100.0%,主动脉骑跨室间隔缺损之上的显示率为96.5%~98.2%。RVOT中,狭窄的肺动脉主干显示率为80.7%~91.2%。Abdomen/stomach中,胃泡及降主动脉的显示率均为100.0%(表3 )。
表3 医师B、C应用5D Heart联合VIS-Assistance®技术分别两次评价法洛四联症患儿各诊断要素的显示率[例(%)] |
| 诊断要素 | 医师B | 医师C | ||
|---|---|---|---|---|
| 第一次 | 第二次 | 第一次 | 第二次 | |
| 3VT | ||||
扩张的主动脉 | 55(96.5) | 54(94.7) | 54(94.7) | 54(94.7) |
狭窄的肺动脉主干 | 54(94.7) | 56(98.2) | 53(93.0) | 55(96.5) |
气管 | 48(84.2) | 47(82.5) | 40(70.2) | 40(70.2) |
上腔静脉 | 52(91.2) | 50(87.7) | 52(91.2) | 49(86.0) |
| 4CV | ||||
4个房室腔 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
房室瓣 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
房室瓣距离 | 53(93.0) | 55(96.5) | 53(93.0) | 54(94.7) |
卵圆孔瓣 | 45(78.9) | 45(78.9) | 45(78.9) | 47(82.5) |
十字交叉 | 54(94.7) | 54(94.7) | 55(96.5) | 55(96.5) |
室间隔 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
调节束 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
| LVOT | ||||
室间隔缺损 | 55(96.5) | 56(98.2) | 55(96.5) | 57(100.0) |
扩张的主动脉 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
主动脉骑跨 | 55(96.5) | 56(98.2) | 55(96.5) | 56(98.2) |
| RVOT | ||||
狭窄的肺动脉主干 | 51(89.5) | 52(91.2) | 46(80.7) | 50(87.7) |
| Abdomen/Stomach | ||||
胃泡 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
降主动脉 | 57(100.0) | 57(100.0) | 57(100.0) | 57(100.0) |
注:3VT为三血管气管切面;4CV为四腔心切面;LVOT为左心室流出道切面;RVOT为右心室流出道切面;Abdomen/Stomach为胃泡切面 |
五、低年资医师应用5D Heart联合VIS-Assistance®技术的重复性检验结果
医师B前后两次各诊断切面评分结果的重复性检验结果显示低年资医师对5个诊断切面的两次评分差异均无统计学意义(均P>0.05),提示低年资医师的评分结果不随检测时间点的不同而不同(表4 )。
表4 医师B应用5D Heart联合VIS-Assistance®技术对法洛四联症患儿各诊断切面进行两次评分的结果[M(P25,P75)] |
| 切面 | 第一次评分 | 第二次评分 | Z值 | P值 |
|---|---|---|---|---|
| 3VT | 2.75(2.50,3.00) | 2.75(2.50,3.00) | -0.228 | 0.820 |
| 4CV | 2.86(2.71,3.00) | 2.86(2.71,3.00) | 0.188 | 0.851 |
| LVOT | 3.00(3.00,3.00) | 3.00(3.00,3.00) | -0.103 | 0.918 |
| RVOT | 3.00(2.00,3.00) | 3.00(2.00,3.00) | -0.746 | 0.456 |
| Abdomen/Stomach | 3.00(3.00,3.00) | 3.00(3.00,3.00) | 0.000 | 1.000 |
注:3VT为三血管气管切面;4CV为四腔心切面;LVOT为左心室流出道切面;RVOT为右心室流出道切面;Abdomen/Stomach为胃泡切面 |
六、高年资医师应用5D Heart联合VIS-Assistance®技术的重复性检验结果
医师C前后两次各诊断切面评分结果的重复性检验结果显示高年资医师对5个诊断切面的两次评分差异均无统计学意义(均P>0.05),提示高年资医师的评分结果不随检测时间点的不同而不同(表5 )。
表5 医师C应用5D Heart联合VIS-Assistance®技术对法洛四联症患儿各诊断切面进行两次评分的结果[M(P25,P75)] |
| 切面 | 第一次评分 | 第二次评分 | Z值 | P值 |
|---|---|---|---|---|
| 3VT | 2.75(2.25,3.00) | 2.75(2.25,3.00) | -0.132 | 0.895 |
| 4CV | 2.86(2.71,3.00) | 2.86(2.71,3.00) | -0.280 | 0.779 |
| LVOT | 3.00(3.00,3.00) | 3.00(3.00,3.00) | -0.535 | 0.593 |
| RVOT | 3.00(2.00,3.00) | 3.00(2.00,3.00) | -0.611 | 0.541 |
| Abdomen/Stomach | 3.00(3.00,3.00) | 3.00(3.00,3.00) | 0.000 | 1.000 |
注:3VT为三血管气管切面;4CV为四腔心切面;LVOT为左心室流出道切面;RVOT为右心室流出道切面;Abdomen/Stomach为胃泡切面 |
七、不同年资的两位医师应用5D Heart联合VIS-Assistance®技术的一致性检验
医师B和C对诊断切面的第一次评分结果显示不同年资的医师对5个诊断切面的评分差异均无统计学意义(均P>0.05),提示评分结果不随医师年资的不同而不同(表6 )。
表6 医师B、C应用5D Heart联合VIS-Assistance®技术对法洛四联症患儿各诊断切面的第一次评分结果[M(P25,P75)] |
| 切面 | 医师B评分 | 医师C评分 | Z值 | P值 |
|---|---|---|---|---|
| 3VT | 2.75(2.50,3.00) | 2.75(2.25,3.00) | -0.132 | 0.895 |
| 4CV | 2.86(2.71,3.00) | 2.86(2.71,3.00) | -0.280 | 0.779 |
| LVOT | 3.00(3.00,3.00) | 3.00(3.00,3.00) | -0.535 | 0.593 |
| RVOT | 3.00(2.00,3.00) | 3.00(2.00,3.00) | -0.611 | 0.541 |
| Abdomen/Stomach | 3.00(3.00,3.00) | 3.00(3.00,3.00) | 0.000 | 1.000 |
注:3VT为三血管气管切面;4CV为四腔心切面;LVOT为左心室流出道切面;RVOT为右心室流出道切面;Abdomen/Stomach为胃泡切面 |
八、妊娠结局
共57例胎儿,8例(14.0%)出生后接受手术治疗,证实为TOF;4例(7.0%)出生后行超声心动图检查证实为TOF。另外32例(56.2%)终止妊娠,13例(22.8%)失访,这45例胎儿依据专家进行的胎儿超声心动图结果作为最终诊断。
讨论
本研究分析不同年资医师应用5D Heart联合VIS-Assistance®新技术,获取经典型TOF胎儿的主要诊断切面及诊断要素的评分结果,探索该技术在胎儿TOF产前诊断中的应用价值。该方法大大简化了获得诊断切面的操作步骤,增加了胎儿TOF的识别率和检出率,有助于疑诊患者接受进一步评估与更为专业的诊断。
此外,本研究表明,当胎儿脊柱位置在除11~1点钟的正前方以外的较大范围时,脊柱的不同位置并不影响TOF图像的显示成功率。Huang等[17]在运用FINE方法筛查34例完全型大动脉转位胎儿时,对于胎儿脊柱的位置扩大为4~8点钟,结果获得合适的STIC容积的成功率为82.4%(28/34)。本研究将脊柱位置的范围进一步扩大,使FINE的应用范围更加广泛。
本研究的局限性在于:此方法目前尚不能替代实时二维超声心动图、彩色多普勒超声及脉冲多普勒超声。原因如下:5D Heart不能评估胎儿心率或心律失常;不能测目标血管的流速,以协助判断肺动脉狭窄;TOF胎儿的血管内径存在异常,本研究采用的5D Heart软件版本尚无法测量主动脉及肺动脉的内径。但随着技术进步,今后有望实现9个切面的彩色多普勒血流的同步显示及定量分析。
综上,5D Heart联合VIS-Assistance®后处理软件可用于TOF的筛查,简化了TOF胎儿心脏检查的流程,减少了检查医师经验和技能的依赖性,使心脏检查的流程更加标准化,对胎儿TOF的5个诊断切面和17个诊断要素的显示率高,有望提高TOF的产前诊断率。