
腹直肌分离是指腹直肌从腹白线向两边分开。腹白线在腹部前方连接左右腹直肌,其宽度称为腹直肌间距(inter-recti distance,IRD),一般用于表示腹直肌分离的距离[1]。妊娠期IRD明显增宽,产后IRD如不能恢复则形成腹直肌分离,首先表现为产后腹围无法恢复,影响美观,可能会引起腰部、盆腔疼痛等不适[2]。随着女性对健康及体形的关注,近年来产后腹直肌生物电刺激治疗广泛开展[3, 4]。目前,按照未婚未育IRD数据,一般认为屈卧位IRD大于两指或2 cm即诊断为腹直肌分离。为了更精确地诊断及干预产后腹直肌分离,迫切需要产后短期内未干预状态下的IRD数据,从而得出IRD医学参考值范围。本研究旨在通过超声测量初步得出产后42~60 d产妇腹直肌间距的参考值范围,为何种情况下需要进行产后腹直肌治疗给出建议。
资料与方法
一、对象
研究对象为2019年8月至2020年8月南京医科大学附属苏州医院产后42~60 d门诊回访产妇,经本人同意签署知情同意书,研究通过本院科研伦理审查。共有126名产妇参与本次研究。纳入标准:(1)年龄为22~40岁的符合法定婚育的产妇;(2)无妊娠高血压、妊娠糖尿病等合并症;(3)自愿配合腹直肌检测。排除标准:(1)既往有腹壁疝、脐尿瘘等疾病史;(2)因其他原因而不能配合腹直肌检测者。
二、仪器与方法
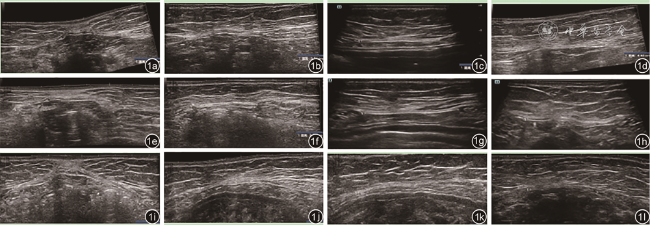
1.仪器和流程:使用超声扫描仪采集静态超声图像(仪器型号迈瑞Resona7,高频超声探头型号L14-5wu,频率5~14 MHz)。受检者取平卧位、屈卧位及站立位3种体位,其中:平卧位为仰卧休息姿势,双腿自然伸直;屈卧位为仰卧双膝弯曲90°,脚平放在检查床上,手臂放在身体两侧,呼气同时用腹部力量使肩膀和头部离开床面,记录整个过程中IRD的最低值;站立位为自然放松站立姿势。于受检者腹中线脐上缘、脐上3 cm、脐上5 cm和脐下3 cm处划线标记,机器设置为肌肉骨骼条件,在3个不同体位时分别将探头置于腹中线四个标记处测量IRD,如IRD过宽,采用宽景成像(图1 )。每个产妇共留取12幅超声图像、获得12个超声测值。
三、统计学分析
所有统计分析均使用SPSS Statistics 25统计学软件。数值变量先以夏皮洛-威尔克法进行正态性检验,年龄、身高为符合正态分布的计量资料,以
±s表示,产后时间、孕前体质量、孕前体质量指数、孕期增重、胎儿体质量、IRD为符合偏态分布的计量资料,以M(QR)表示。采用2组独立数据秩和检验比较经阴道分娩组与剖宫产分娩组、第一胎与非第一胎组在不同体位的不同脐水平时IRD的差异。分类变量以例(%)表示。P<0.05为差异具有统计学意义。偏态分布数值变量的参考值范围以第20百分位数和第80百分位数定义。

{kind=link}
{kind=link}
结果
一、基本临床资料
本研究共纳入126名产后42~60 d女性,受检者年龄为(29±4)岁,身高为(1.61±0.05)m,产后时间为48(43,56)d,孕前体质量53(50,58)kg,孕前体质量指数为20.58(19.09,22.06)kg/m2,孕期增重14(11,17)kg,胎儿体质量为3.4(3.2,3.7)kg;经阴道分娩89例(70.6%,89/126),剖宫产分娩37例(29.4%,37/126);第一胎72例(57.1%,72/126),非第一胎54例(42.9%,54/126)。
二、分娩方式与胎次对IRD的影响分析
3个不同体位中,脐上缘、脐上3 cm、脐上5 cm、脐下3 cm的IRD均依次递减。脐上缘、脐上3 cm、脐上5 cm IRD在站立位时最宽,屈卧位时最窄;脐下3 cm的IRD在平卧位最宽,站立位最窄。经阴道分娩组与剖宫产分娩组在不同体位的不同脐水平时IRD比较,差异均具有统计学意义(P均<0.05,表1 )。第一胎与非第一胎组在不同体位的不同脐水平时IRD比较,差异均无统计学意义(P均>0.05,表2 )。
表1 不同分娩方式组产妇不同体位的不同脐水平腹直肌间距的比较[mm,M(QR)] |
| 组别 | 例数 | 平卧位 | |||
|---|---|---|---|---|---|
| 脐上缘 | 脐上3 cm | 脐上5 cm | 脐下3 cm | ||
| 经阴道分娩组 | 89 | 25.00(20.15,33.20) | 20.00(15.45,27.35) | 14.70(12.00,20.55) | 9.10(4.55,13.65) |
| 剖宫产分娩组 | 37 | 32.80(27.10,40.05) | 26.60(21.15,31.20) | 20.20(15.55,27.05) | 17.00(8.15,22.95) |
| Z值 | -3.27 | -3.24 | -3.04 | -3.60 | |
| P值 | 0.001 | 0.001 | 0.002 | <0.001 | |
| 组别 | 例数 | 屈卧位 | |||
| 脐上缘 | 脐上3 cm | 脐上5 cm | 脐下3 cm | ||
| 经阴道分娩组 | 89 | 21.40(17.60,28.90) | 17.10(14.25,22.85) | 13.70(9.85,18.30) | 6.60(3.15,10.50) |
| 剖宫产分娩组 | 37 | 26.90(20.80,34.60) | 23.40(18.40,27.80) | 18.80(13.80,24.50) | 9.80(6.70,18.00) |
| Z值 | -2.65 | -3.27 | -3.51 | -2.88 | |
| P值 | 0.008 | 0.001 | <0.001 | 0.004 | |
| 组别 | 例数 | 站立位 | |||
| 脐上缘 | 脐上3 cm | 脐上5 cm | 脐下3 cm | ||
| 经阴道分娩组 | 89 | 30.90(20.35,37.95) | 24.10(18.25,31.65) | 18.20(12.80,23.55) | 0.00(0.00,7.45) |
| 剖宫产分娩组 | 37 | 37.90(29.35,44.65) | 31.40(22.55,38.00) | 23.60(18.65,31.70) | 8.70(0.00,16.60) |
| Z值 | -3.31 | -2.82 | -3.24 | -3.48 | |
| P值 | 0.001 | 0.005 | 0.001 | <0.001 | |
表2 不同胎次组产妇不同体位的不同脐水平腹直肌间距的比较[mm,M(QR)] |
| 组别 | 例数 | 平卧位 | |||
|---|---|---|---|---|---|
| 脐上缘 | 脐上3 cm | 脐上5 cm | 脐下3 cm | ||
| 第一胎 | 72 | 28.15(21.10,37.50) | 21.35(16.43,28.45) | 16.45(12.60,22.35) | 9.95(7.15,16.98) |
| 非第一胎 | 54 | 29.70(21.25,35.05) | 21.85(16.70,29.25) | 17.20(12.13,22.78) | 10.20(4.35,16.85) |
| Z值 | -0.11 | -0.29 | -0.05 | -0.38 | |
| P值 | 0.912 | 0.771 | 0.963 | 0.702 | |
| 组别 | 例数 | 屈卧位 | |||
| 脐上缘 | 脐上3 cm | 脐上5 cm | 脐下3 cm | ||
| 第一胎 | 72 | 22.40(17.75,29.70) | 19.10(15.30,25.45) | 14.60(11.70,19.10) | 7.80(4.38,12.03) |
| 非第一胎 | 54 | 25.40(20.15,31.70) | 18.65(15.68,27.13) | 15.55(10.68,20.13) | 7.45(3.40,12.18) |
| Z值 | -1.45 | -0.47 | -0.19 | -0.07 | |
| P值 | 0.148 | 0.641 | 0.848 | 0.947 | |
| 组别 | 例数 | 站立位 | |||
| 脐上缘 | 脐上3 cm | 脐上5 cm | 脐下3 cm | ||
| 第一胎 | 72 | 31.65(25.33,39.48) | 24.85(20.80,33.63) | 18.80(13.65,26.63) | 3.00(0.00,10.68) |
| 非第一胎 | 54 | 32.75(24.73,39.78) | 27.20(18.05,36.50) | 20.30(13.03,29.00) | 2.30(0.00,9.10) |
| Z值 | -0.15 | -0.42 | -0.29 | -0.42 | |
| P值 | 0.884 | 0.677 | 0.773 | 0.674 | |
三、产后IRD的参考值范围
由第二部分结果可知,不同分娩方式的产后IRD差异具有统计学意义,所以产后IRD的参考值范围以P20~P80拟定,并根据分娩方式不同进行分组。
经阴道分娩组3个体位4个测量点P20~P80分别为19.60~38.30 mm、15.10~28.80 mm、11.00~21.50 mm、2.70~15.50 mm、16.70~30.90 mm、12.90~26.30 mm、9.20~19.90 mm、1.90~12.00 mm、19.00~39.10 mm、15.90~35.50 mm、11.20~28.50 mm、0.00~8.60 mm。剖宫产分娩组3个体位4个测量点P20~P80分别为25.92~44.04 mm、19.78~32.44 mm、14.94~28.76 mm、7.78~24.88 mm、20.12~36.68 mm、17.20~28.44 mm、13.38~26.24 mm、4.08~18.62 mm、28.80~45.68 mm、21.18~40.38 mm、18.04~33.70 mm、0.00~18.62 mm(表3 )。
表3 不同分娩方式产后腹直肌间距的不同百分位数数值(mm) |
| 组别 | 第5百分位数 | 第10百分位数 | 第20百分位数 | 第50百分位数 | 第80百分位数 | 第90百分位数 | 第95百分位数 |
|---|---|---|---|---|---|---|---|
| 经阴道分娩组 | |||||||
平卧位脐上缘 | 13.45 | 16.60 | 19.60 | 25.00 | 38.30 | 43.20 | 49.90 |
平卧位脐上3 cm | 8.70 | 10.80 | 15.10 | 20.00 | 28.80 | 34.20 | 40.10 |
平卧位脐上5 cm | 6.60 | 8.80 | 11.00 | 14.70 | 21.50 | 30.80 | 38.85 |
平卧位脐下3 cm | 0.00 | 0.00 | 2.70 | 9.10 | 15.50 | 17.90 | 23.25 |
屈卧位脐上缘 | 10.25 | 12.30 | 16.70 | 21.40 | 30.90 | 33.70 | 43.20 |
屈卧位脐上3 cm | 8.50 | 9.70 | 12.90 | 17.10 | 26.30 | 32.20 | 34.10 |
屈卧位脐上5 cm | 5.20 | 7.60 | 9.20 | 13.70 | 19.90 | 25.00 | 32.50 |
屈卧位脐下3 cm | 0.00 | 0.00 | 1.90 | 6.60 | 12.00 | 18.80 | 22.45 |
站立位脐上缘 | 10.30 | 14.30 | 19.00 | 30.90 | 39.10 | 46.30 | 51.75 |
站立位脐上3 cm | 9.85 | 13.10 | 15.90 | 24.10 | 35.50 | 40.40 | 48.20 |
站立位脐上5 cm | 8.20 | 9.40 | 11.20 | 18.20 | 28.50 | 34.80 | 40.60 |
站立位脐下3 cm | 0.00 | 0.00 | 0.00 | 0.00 | 8.60 | 12.30 | 13.55 |
| 剖宫产分娩组 | |||||||
平卧位脐上缘 | 20.02 | 21.94 | 25.92 | 32.80 | 44.04 | 47.78 | 49.90 |
平卧位脐上3 cm | 14.18 | 15.98 | 19.78 | 26.60 | 32.44 | 39.60 | 43.72 |
平卧位脐上5 cm | 10.70 | 11.86 | 14.94 | 20.20 | 28.76 | 32.52 | 34.44 |
平卧位脐下3 cm | 0.00 | 0.00 | 7.78 | 17.00 | 24.88 | 28.34 | 39.49 |
屈卧位脐上缘 | 14.04 | 16.36 | 20.12 | 26.90 | 36.68 | 40.10 | 43.88 |
屈卧位脐上3 cm | 13.76 | 16.26 | 17.2 | 23.40 | 28.44 | 30.50 | 30.90 |
屈卧位脐上5 cm | 8.65 | 11.98 | 13.38 | 18.80 | 26.24 | 29.72 | 31.44 |
屈卧位脐下3 cm | 0.00 | 0.00 | 4.08 | 9.80 | 18.62 | 21.34 | 25.61 |
站立位脐上缘 | 18.82 | 23.30 | 28.80 | 37.90 | 45.68 | 54.52 | 59.81 |
站立位脐上3 cm | 16.11 | 16.62 | 21.18 | 31.40 | 40.38 | 46.80 | 51.76 |
站立位脐上5 cm | 12.47 | 12.80 | 18.04 | 23.60 | 33.70 | 37.20 | 41.59 |
站立位脐下3 cm | 0.00 | 0.00 | 0.00 | 8.70 | 18.62 | 22.62 | 28.20 |
讨论
怀孕期间,随着胎儿增大,孕妇的腹内压力增加以及激素的影响使腹直肌松弛,产后短期内IRD肯定比未育女性宽,如果参照未育女性的诊断标准,会导致产后腹直肌分离的过度诊断。部分产后短期内IRD>2 cm的经产妇随着产后时间推移,IRD会逐渐恢复至正常水平;同时,按照2 cm的诊断标准,在产后12个月产后腹直肌分离的发病率依然可以达到30%[10]。产后短期内是腹直肌分离的最佳治疗时机,迫切需要一个精确的诊断标准,使得产后腹直肌分离既不过度诊断,也不会使那些需要即刻治疗的产妇错过最佳治疗时机。
既往研究[13]表明,腹前壁正中线不同测量点、不同体位的IRD不同。为了获得更具有代表性的数据,本研究通过超声测量法量取较多的测量点及不同体位的IRD。笔者在测量时发现,屈卧位腹直肌边缘在静态图像中较平卧位、站立位更清晰;同时,测量屈卧位腹直肌边缘可以动态观察,更容易获得腹直肌内缘的确切位置。有研究[5]中,屈卧位腹直肌测量是平卧位时经产妇头下垫固定高度的枕头,收腹时患者吐气同时将枕头抽离,确保每个患者头部离开床面的距离都是相等的;也有研究[14]并没有提及具体身体抬高的高度或弯曲的角度。由于经产妇上半身长度不同,离开床面相同的高度但身体屈曲的角度并不相同,所以腹肌收缩的程度也不相同;另外,经产妇的腹肌力量不同,有些经产妇在吐气腹肌用力折叠身体的过程中IRD先缩短,但过了某一临界点,IRD随着屈曲程度增加反而逐渐增加。因此,为了规避这些不确定因素,笔者将屈卧位每个经产妇IRD的最小值作为屈卧位的测量数据。
本研究发现,剖宫产组所有测量点IRD均高于经阴道分娩组,这也与既往的研究较为一致[15, 16, 17]。这可能与剖宫产手术分娩时腹直肌被撕拉造成直接损伤有关。在临床诊断中,IRD触诊或测量一般是以屈卧位为标准[11,18],根据本研究结果,20 mm位于屈卧位经阴道分娩组第50百分位数处、剖宫产组第20百分位数处。显然,以屈卧位任何测量点触诊大于2指或测量>20 mm诊断产后腹直肌分离造成了过度诊断。因此,在产后40~60 d时采用超声测量IRD,可以初步以第20百分位数和第80百分位数定义IRD的“正常”宽度。根据IRD百分位数结果,屈卧位最大IRD超过30.90 mm(经阴道分娩)、36.68 mm(剖宫产分娩)时表明产妇的IRD已经超过80%的产妇,建议进行进一步的治疗或康复手段。
本文的不足之处在于样本量有限,同时,这些愿意参加研究的产妇都是了解产后腹直肌分离的,这些数据更能代表这一认知水平产妇的总体情况。所以笔者将增加健康宣教力度,让更多认知层次的产妇愿意接受IRD检测,力求获得更全面的产后42~60 d产妇的IRD数据,在样本量保证的基础上制定出更准确的产后IRD医学参考值范围。
本研究为观察性研究,研究因素与结论的关系是探索性的,其因果关系需要进一步通过前瞻性研究予以确认。必须关注那些屈卧位腹直肌最大间距小于第80百分位数的经产妇,有必要将所有产妇纳入研究,以IRD第80百分位数为界分为腹直肌分离组和正常组,根据产妇意愿,组内再分为电刺激治疗组和对照组,随访4组IRD恢复情况的差异,这也是笔者今后的研究方向。