
超声检查是甲状腺结节检出及良恶性诊断的首要检查方法[7, 8, 9]。根据美国放射学会(American College of Radiology,ACR)颁布的甲状腺影像报告和数据系统(thyroid imaging reporting and data system,TI-RADS)数据,4类甲状腺结节的恶性概率为5%~20%,结节最大径≥1.5 cm时建议行超声引导下细针穿刺活检(fine-needle aspiration biopsy,FNA),结节最大径≥1 cm时建议定期随访[10]。而我国TI-RADS 4类结节患者因心理负担过重,大多选择超声引导下穿刺活检以明确诊断。超声检查具有便携、无辐射、患者耐受性良好等优点,但是对于最大径≤1 cm的甲状腺结节,因其体积小,超声图像特征的判读和诊断对操作者依赖性强[11, 12],导致不同年资医师的诊断结果存在较大差异,其中低年资住院医师诊断效能较低。
资料与方法
一、对象
连续选取2021年3~4月于解放军总医院第一医学中心超声诊断科行甲状腺超声检查及超声引导穿刺活检或切除手术的360例患者(400个甲状腺结节)。纳入标准:(1)接受常规超声检查和S-detect技术扫查;(2)结节最大直径≤1 cm;(3)ACR TI-RADS 4类;(4)病理诊断结果明确。排除标准:于本院超声检查前已知病理结果。最终纳入133例患者(133个甲状腺结节)。
良性甲状腺结节诊断标准:(1)超声引导下FNA结果为Bethesda Ⅱ类结节[16];(2)超声引导下粗针穿刺活检或手术病理结果为良性。恶性甲状腺结节诊断标准:(1)FNA结果为Bethesda Ⅵ类结节;(2)FNA结果为Bethesda Ⅴ类结节且BRAF(V600E)基因突变;(3)超声引导下粗针穿刺活检或手术病理结果为恶性。
二、仪器与方法
1. 仪器:采用Samsung RS85A型彩色多普勒超声诊断仪,L3-12A线阵探头,探头频率为3.0~12.0 MHz。
2. 方法:患者取仰卧位,充分暴露颈部,颈部转向对侧。由1名超声医师(从事甲状腺超声检查工作4年)进行常规甲状腺超声检查,每个甲状腺结节留取包含病灶最大径线且病灶特征最典型的二维超声图像及彩色多普勒血流图像。动态扫查甲状腺后,选取病灶特征最典型的纵切面并冻结图像,选择S-detect模式,人工定位结节区域,S-detect对病灶边界进行自动识别并作出“良性可能”或“恶性可能”的二分类诊断结果,留存诊断报告图像。
所有患者均采用上述检查方式,超声图像及S-detect诊断报告存储于数据库。由2名超声住院医师(具有2年甲状腺超声诊断经验)共同读取图像数据并进行甲状腺结节良恶性的诊断,当2人意见不统一时,进行协商以达成一致结果。2位医师事先均不知晓病理结果。
研究步骤分2个阶段进行:(1)2名住院医师共同阅读所有甲状腺结节的二维超声图像(每个结节提供1幅病灶特征最典型的纵切图),共133幅超声图像,对每个结节进行仔细阅读后,进行“良性可能”或“恶性可能”的二分类诊断;(2)2周后,该2名住院医师共同阅读所有甲状腺结节的二维超声图像及S-detect诊断报告(每个结节提供1幅病灶特征最典型的纵切图及S-detect对该图的诊断报告),综合考虑后进行“良性可能”或“恶性可能”的二分类诊断。
三、统计学分析
采用SPSS 23.0及Medcalc 20.0统计软件进行统计学分析。患者年龄、结节最大直径为符合正态分布的计量资料,以
±s表示。以病理结果作为金标准,分别计算常规超声、S-detect技术和两者联合鉴别诊断甲状腺微小乳头状癌的敏感度、特异度、准确性、阳性预测值及阴性预测值。采用McNemar检验比较3种诊断模式的诊断效能(敏感度、特异度及准确性)的差异。绘制3种诊断方法的受试者操作特征(receiver operating characteristic,ROC)曲线并计算曲线下面积(area under curve,AUC),采用Delong检验比较三者之间的差异。P<0.05为差异具有统计学差异。

结果
一、一般临床情况
133例患者共133个甲状腺结节,其中男性患者22例,女性患者111例,年龄为(42.8±9.7)岁(范围为23~72岁),结节最大径为(0.70±0.19)cm(范围为0.30~1.00 cm)。其中甲状腺良性结节21个(15.8%,21/133),恶性结节112个(84.2%,112/133),均为甲状腺乳头状癌(表1 )。
表1 133例甲状腺结节患者一般临床资料 |
| 特征 | 良性 | 恶性 |
|---|---|---|
| 患者(例) | 21 | 112 |
| 结节(个) | 21 | 112 |
| 男性/女性 | 2/19 | 20/92 |
| 年龄(岁, ±s) | 47.57±6.67(37~56) | 41.93±9.93(23~72) |
| 结节最大直径(cm, ±s) | 0.75±0.20(0.36~0.98) | 0.69±0.18(0.30~1.00) |

注:年龄和结节最大直径括号内为范围值 |
二、住院医师、S-detect技术和两者联合的诊断效能
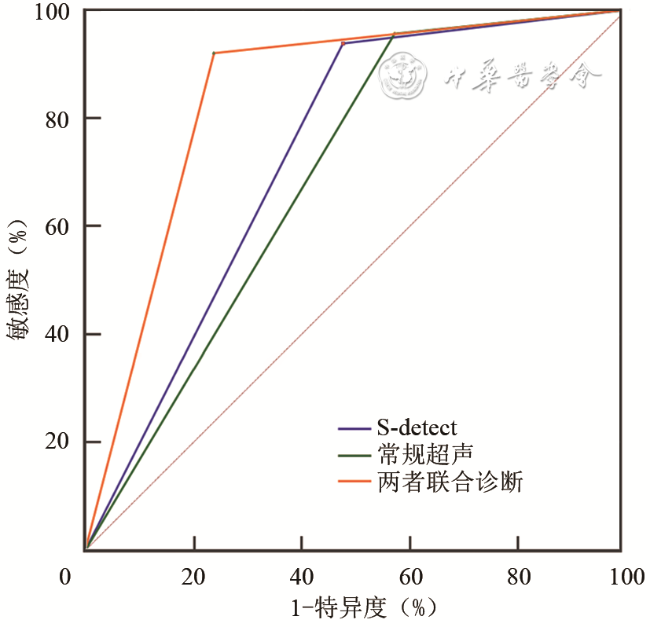
以病理结果为金标准鉴别TI-RADS 4类最大径≤1 cm甲状腺结节良恶性,常规超声、S-detect技术(图1 )和两者联合诊断(图2 )3种诊断方法中,两者联合诊断的准确性、特异度均高于常规超声或S-detect技术单独诊断的准确性和特异度,其中联合诊断与常规超声诊断的特异度差异具有统计学意义(P<0.05);常规超声诊断的AUC低于S-detect技术,差异无统计学意义(P>0.05);联合诊断的AUC高于常规超声或S-detect技术,差异均具有统计学意义(P均<0.05;表2 、3 ,图3 )。
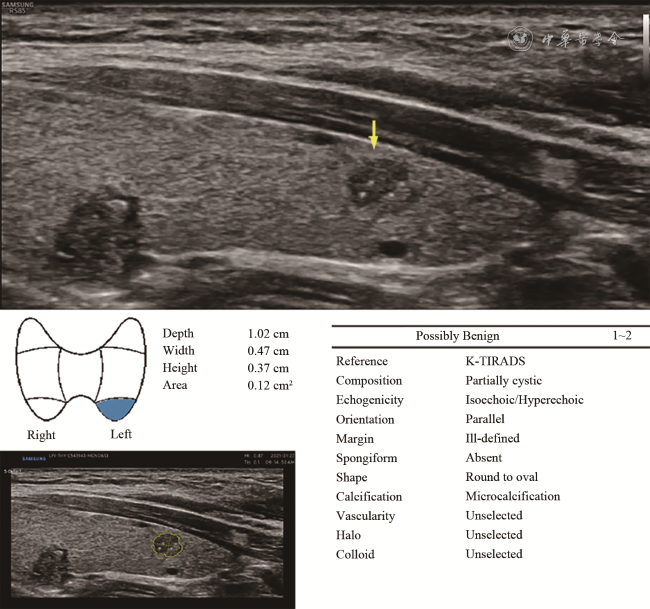
图1 S-detect技术鉴别最大径≤1 cm甲状腺结节良恶性的漏诊病例。甲状腺左叶下等/稍低回声实性结节,边界模糊,形态欠规则,内可见多发点状强回声,S-detect技术诊断为良性可能,病理结果为甲状腺乳头状癌 |
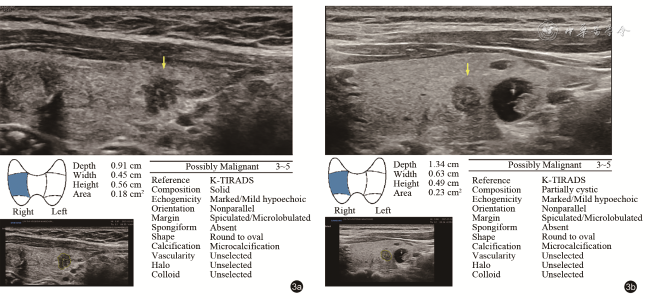
图2 S-detect技术与常规超声联合诊断最大径≤1 cm甲状腺结节良恶性的正确病例。图a示甲状腺右叶下低回声实性结节,边界模糊,形态欠规则,常规超声诊断为良性可能,S-detect技术诊断为恶性可能,病理结果为甲状腺乳头状癌;图b示甲状腺右叶中部稍低回声结节,边界不清,形态尚规则,常规超声诊断为良性可能,S-detect技术诊断为恶性可能,病理结果为甲状腺乳头状癌 |
表2 常规超声、S-detect技术及两者联合诊断结果 |
| 诊断方法 | 病理结果 | 合计 | |
|---|---|---|---|
| 良性 | 恶性 | ||
| 常规超声 | |||
| 良性 | 9 | 5 | 14 |
| 恶性 | 12 | 107 | 119 |
| S-detect技术 | |||
| 良性 | 11 | 7 | 18 |
| 恶性 | 10 | 105 | 115 |
| 联合诊断 | |||
| 良性 | 16 | 9 | 25 |
| 恶性 | 5 | 103 | 108 |
| 合计 | 21 | 112 | |
表3 常规超声、S-detect技术及两者联合诊断TI-RADS 4类最大径≤1 cm甲状腺结节良恶性的诊断效能 |
| 诊断方法 | 曲线下面积 | 准确性(%) | 敏感度(%) | 特异度(%) | 阳性预测值(%) | 阴性预测值(%) |
|---|---|---|---|---|---|---|
| 常规超声 | 0.692(0.606~0.769) | 88.0(81.5~93.0) | 95.5(89.9~98.5) | 42.9(21.8~66.0) | 89.9(84.4~95.4) | 64.3(35.6~93.0) |
| S-detect技术 | 0.731(0.647~0.804) | 87.2(81.5~93.0) | 93.8(89.2~98.3) | 52.4(29.1~75.7) | 91.3(86.1~96.5) | 61.1(36.2~86.1) |
| 联合诊断 | 0.841(0.767~0.898) | 89.5(84.2~94.8) | 92.0(85.3~96.3) | 76.2(52.8~91.8) | 95.4(91.3~99.4) | 64.0(43.8~84.2) |
| P值a | 0.522 | 1.000 | 0.754 | 0.687 | - | - |
| P值b | 0.007 | 0.648 | 0.388 | 0.016 | - | - |
| P值c | 0.028 | 0.629 | 0.774 | 0.063 | - | - |
注:TI-RADS为甲状腺影像报告和数据系统;a为S-detect技术与常规超声比较,b为联合诊断与常规超声比较,c为联合诊断与S-detect技术比较;“-”表示未进行统计比较,括号内数据为95%可信区间 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
讨论
S-detect技术采用基于卷积神经网络的深度学习算法,能够自动识别甲状腺结节的边界、形态、回声、钙化等特征,为结节TI-RADS分类及良恶性诊断提供参考。既往研究报道,S-detect技术诊断甲状腺恶性肿瘤具有较高的敏感度(80.0%~91.3%)[19, 20, 21, 22],一项Meta分析显示S-detect技术诊断合并敏感度和AUC分别为84%和0.89[23],本研究中,S-detect技术诊断≤1 cm TI-RADS 4类甲状腺结节的敏感度(93.8%)和AUC(0.731)较高,与既往研究结果一致。但是在上述Meta分析中,S-detect诊断的合并特异度可达71%,本研究中S-detect诊断的特异度为52.4%,研究结果的差异可能与纳入样本量和疾病种类有关:本研究纳入恶性甲状腺结节数量较良性结节多,一部分良性特征明显但无病理结果的良性结节被排除,导致特异度降低。虽然不同研究报道S-detect技术对甲状腺结节良恶性的诊断效能存在一定的差异,但其较高的敏感度和准确性可辅助临床医师筛查出甲状腺微小癌,具有重要的临床应用价值。
本研究结果显示,单独应用S-detect技术诊断甲状腺微小乳头状癌的准确性和敏感度稍低于常规超声检查(87.2% vs 88.0%,93.8% vs 95.5%),提示对于最大径≤1 cm的甲状腺结节,单独应用S-detect技术的诊断效能尚不理想。例如其中部分甲状腺结节超声图像具有恶性特征,如实性低回声、微钙化、边缘成角或分叶等,应用S-detect技术诊断为“良性可能”而被漏诊,手术病理证实为甲状腺乳头状癌;部分结节超声图像提示边界模糊、实性、低回声等,S-detect技术诊断为“恶性可能”被误诊,组织学病理诊断为炎性改变。分析漏诊、误诊原因,考虑与S-detect技术对结节部分超声特征识别欠佳相关,既往研究报道AI系统与高年资医师描述甲状腺结节超声特征的一致性不高,尤其是对结节边界、钙化的识别能力欠佳,仍需要进一步提高[24]。
本研究以最大径≤1 cm的甲状腺结节为研究对象,S-detect技术与常规超声联合诊断的AUC、准确性和特异度均较单独应用常规超声及单独应用S-detect技术有所提高,其中AUC的提高差异具有统计学意义,这与既往研究结果一致[21, 22,24],表明S-detect技术可明显提高低年资医师的诊断效能。本研究中,特异度和阳性预测 值的提升可提高甲状腺良性结节的诊断能力,降低了不必要的穿刺活检数量。S-detect技术与常规超声联合诊断甲状腺微小乳头状癌的敏感度较单独应用常规超声稍有下降(92.0% vs 95.5%),一小部分甲状腺微小癌被误诊为良性,相关文献报道甲状腺微小癌可进行积极检测[25],因此,敏感度小幅度降低可被允许。S-detect技术与常规超声联合诊断的优势有以下几点:首先,S-detect技术基于深度学习方法,已经学习大量超声图像,弥补了临床医师某些经验的不足,降低操作者依赖性,减少主观错误;其次,常规超声通过多方位、多切面、多角度扫查,可详细了解病灶的内部情况及其与周围组织的关系,提高对甲状腺微小结节良恶性的辨识率;此外,常规超声诊断过程中,医师通过询问病史,紧密结合临床,可提高鉴别诊断能力。
本研究的不足:本研究纳入拟行超声引导下穿刺活检或甲状腺切除术前行超声检查的甲状腺结节患者,因此,恶性结节数量较多,在不同人群中S-detect诊断效能可能有所差异。其次,本研究样本量较小,统计结果可能存在偏差;S-detect技术是基于灰阶超声图像信息,未纳入彩色多普勒超声、弹性成像等相关信息。
综上所述,S-detect技术是一种新型AI,用以辅助住院医师可进一步提高对≤1 cm TI-RADS 4类甲状腺结节良恶性的诊断效能,减少不必要的穿刺活检,具有重要临床应用价值。