
胸锁乳突肌是侧颈部的主要肌肉之一,为颈部淋巴结分区的重要解剖标志,参与深吸气过程,并对头颈部的运动和姿势的维持具有重要作用[1]。胸锁乳突肌可发生肌性斜颈、肿瘤、肌炎、结核等病变,且近年来口腔颌面部病变手术切除后使用胸锁乳突肌瓣填充术腔以最大限度地修复缺损处外观与功能的需求日益增多,术前了解患者胸锁乳突肌精细解剖情况有助于更好地完成手术规划。目前,国内尚未有文献报道使用超声观察正常胸锁乳突肌的内部精细结构,本研究通过高频超声观察并测量正常胸锁乳突肌的内部精细结构,探讨高频超声评价胸锁乳突肌内部精细结构的可行性,为胸锁乳突肌的病变诊断及精准肌瓣选择提供依据。
资料与方法
一、对象
2022年5月至6月征集健康志愿者91人,其中男性48人,女性43人;均无颈部外伤、手术、肿瘤、放疗史,无颈部肌肉锻炼史。记录其年龄、身高、体质量、体质量指数(body mass index,BMI)、优势手。
二、仪器与方法
1名具有肌肉骨骼超声检查经验10年以上的超声医师,应用三星RS80A超声诊断仪,采用L3-12高频探头(频率范围3~12 MHz),选择肌肉骨骼预设条件进行扫查。所有受检者取去枕平卧中立位,充分暴露颈部,使用足量耦合剂,探头轻置于皮肤表面、避免加压。扫查双侧胸锁乳突肌全长,获取肌肉的长轴和短轴切面声像图,观察其全程形态、内部回声、有无解剖变异,并垂直于皮肤测量以下数据(所有数据均测量3次,取平均值为最终结果):乳突与胸锁关节连线中点处胸锁乳突肌总厚度、各肌束厚度,锁骨上缘、胸骨上缘止点处宽度,距锁骨、胸骨止点上缘1 cm处内部腱膜宽度、厚度,锁骨头、胸骨头肌束内腱膜长度。若有止点处变异,则宽度为总和、厚度取最大值。
三、统计学分析
使用SPSS 25.0统计软件进行统计学分析。本研究测值均为符合正态分布的计量资料,采用
±s表示,2组间比较(左侧与右侧、男性与女性)采用独立样本t检验,胸锁乳突肌各部分厚度多组间比较采用方差分析;因左侧、右侧胸锁乳突肌各部分厚度测值方差不齐(方差齐性检验P均=0.001),故使用塔姆黑尼法两两比较各部分厚度测值差异;使用Pearson相关分析检验胸锁乳突肌总厚度、各部分厚度与BMI是否相关。P<0.05为差异具有统计学意义。

结果
一、一般临床资料
所有受检者均为右利手。受检者年龄为(37.31±8.96)岁(范围21~55岁)。男性与女性年龄比较,差异无统计学意义(P>0.05),男性身高、体质量、体质量指数高于女性,差异均具有统计学意义(P均<0.05,表1 )。
表1 不同性别分组一般资料比较结果( |

| 组别 | 人数 | 年龄(岁) | 身高(m) | 体质量(kg) | 体质量指数 |
|---|---|---|---|---|---|
| 男性组 | 48 | 37.42±8.72 | 1.73±0.07 | 72.84±11.23 | 24.43±2.92 |
| 女性组 | 43 | 37.19±9.32 | 1.63±0.06 | 56.20±7.99 | 21.28±2.75 |
| t值 | -0.122 | -7.290 | -8.056 | -5.282 | |
| P值 | 0.903 | <0.001 | <0.001 | <0.001 |
二、正常胸锁乳突肌的超声形态及变异
91名健康志愿者的双侧胸锁乳突肌全程及内部结构均可清晰显示。
胸锁乳突肌的肌腹与肌腱的回声与其他骨骼肌类似:肌外膜为高回声,肌束为低回声,肌腱和肌内腱膜呈高回声带。该肌肉双侧对称,两头薄,中间厚,外形光滑规则,没有局部隆起或凹陷。
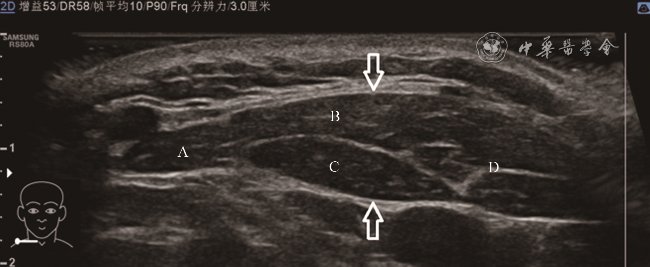
胸锁乳突肌的头侧止点为乳突和上项线,足侧止点为胸骨和锁骨上缘。向头侧追踪时,可见乳突止点附近肌腹内出现高回声腱膜成分后逐渐移行为肌腱,并呈“鸟嘴样”止于乳突;枕骨止点附近肌腹移行为高回声腱膜后止于上项线。向足侧追踪时,可见从上项线发出的腱膜和从乳突发出的肌腱在移行为肌腹后均在中下部分开,内部出现高回声腱膜成分并逐渐移行为肌腱,分别止于锁骨的前上缘和胸骨上部的前缘,即胸锁乳突肌由4个部分组成(图1 ),分别为枕骨锁骨束、枕骨胸骨束、乳突锁骨束、乳突胸骨束。在胸锁乳突肌中段水平,枕骨锁骨束位于最外侧,乳突胸骨束位于最内侧,枕骨胸骨束和乳突锁骨束则分别位于中间的浅层和深层。该4个部分在空间上为紧邻走行,乳突锁骨束与其他部分之间的分界十分清晰,为平滑规则的高回声线,而枕骨胸骨束和乳突胸骨束之间的分界较为清晰。
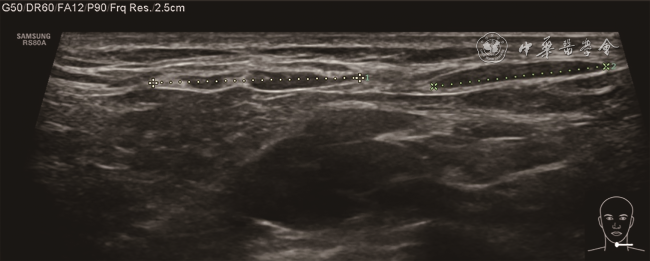
91人中有7例(7.69%)可见解剖变异,均为单侧发生的锁骨止点变异:2个分开的肌腱止于锁骨上缘处(图2 )。其中左侧3例(女性3例,男性0例),右侧4例(女性3例,男性1例)。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
三、正常胸锁乳突肌的测值
乳突与胸锁关节连线中点处胸锁乳突肌总厚度、4个部分(乳突锁骨束、乳突胸骨束、枕骨锁骨束、枕骨胸骨束)厚度测量值分别为(0.90±0.16)cm、(0.54±0.13)cm、(0.68±0.14)cm、(0.40±0.10)cm、(0.28±0.09)cm。BMI与胸锁乳突肌总厚度及乳突锁骨束、乳突胸骨束、枕骨锁骨束、枕骨胸骨束厚度的Pearson相关系数分别为0.371、0.322、0.333、0.286、0.286(P均<0.001)。
左侧与右侧胸锁乳突肌总厚度、乳突锁骨束厚度、乳突胸骨束厚度、枕骨锁骨束厚度、枕骨胸骨束厚度测值比较,差异均无统计学意义(P均>0.05,表2 )。使用方差分析比较左侧、右侧4个部分厚度的测值差异,左侧、右侧各部分厚度差异均具有统计学意义(F=195.711,P<0.001;F=209.486,P<0.001);左侧、右侧各部分厚度测值两两比较,组间差异均具有统计学意义(P均<0.001,表2 )。
表2 健康志愿者双侧胸锁乳突肌总厚度及4个部分厚度测量值比较(cm, |
| 组别 | 人数 | 胸锁乳突肌总厚度 | 乳突锁骨束厚度 | 乳突胸骨束厚度 | 枕骨锁骨束厚度 | 枕骨胸骨束厚度 |
|---|---|---|---|---|---|---|
| 左侧组 | 91 | 0.91±0.16 | 0.53±0.13 | 0.68±0.14a | 0.39±0.10a,b | 0.29±0.09a,b,c |
| 右侧组 | 91 | 0.89±0.17 | 0.54±0.13 | 0.68±0.14a | 0.41±0.10a,b | 0.27±0.09a,b,c |
| t值 | 0.595 | -0.699 | -0.079 | -0.973 | 1.197 | |
| P值 | 0.552 | 0.485 | 0.937 | 0.332 | 0.233 |
注:a与乳突锁骨束厚度比较,b与乳突胸骨束厚度比较,c与枕骨锁骨束厚度比较,差异均具有统计学意义(P均<0.001) |
男性与女性胸锁乳突肌总厚度、乳突锁骨束厚度、乳突胸骨束厚度、枕骨锁骨束厚度、枕骨胸骨束厚度测值比较,差异均具有统计学意义(P均<0.05,表3 )。
表3 不同性别健康志愿者胸锁乳突肌总厚度及4个部分厚度测量值比较(cm, |
| 组别 | 人数 | 胸锁乳突肌总厚度 | 乳突锁骨束厚度 | 乳突胸骨束厚度 | 枕骨锁骨束厚度 | 枕骨胸骨束厚度 |
|---|---|---|---|---|---|---|
| 男性组 | 48 | 0.98±0.15 | 0.60±0.12 | 0.74±0.14 | 0.44±0.11 | 0.29±0.08 |
| 女性组 | 43 | 0.81±0.12 | 0.46±0.08 | 0.62±0.11 | 0.36±0.07 | 0.26±0.10 |
| t值 | -8.366 | -9.529 | -6.772 | -6.430 | -2.558 | |
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | 0.011 |
锁骨上缘、胸骨上缘止点处宽度,距锁骨、胸骨止点上缘1 cm处内部腱膜宽度、厚度,锁骨头、胸骨头肌束内腱膜长度的双侧测值比较,差异均无统计学意义(P均>0.05,表4 )。除距锁骨、胸骨止点上缘1 cm处内部腱膜厚度及胸骨束腱膜长度外,上述测值男性组和女性组比较,差异均具有统计学意义(P均<0.05,表5 )。
表4 健康志愿者双侧胸锁乳突肌内部结构测量平均值(cm, |
| 项目 | 左侧组 | 右侧组 | t值 | P值 |
|---|---|---|---|---|
| 锁骨束止点宽度 | 3.05±0.71 | 3.13±0.71 | -0.759 | 0.449 |
| 锁骨束腱膜宽度 | 0.84±0.48 | 0.81±0.47 | 0.485 | 0.628 |
| 锁骨束腱膜厚度 | 0.08±0.03 | 0.08±0.04 | 0.140 | 0.889 |
| 胸骨束止点宽度 | 0.86±0.15 | 0.88±0.14 | -0.763 | 0.446 |
| 胸骨束腱膜宽度 | 0.69±0.23 | 0.74±0.24 | 1.249 | 0.213 |
| 胸骨束腱膜厚度 | 0.12±0.06 | 0.13±0.06 | 0.609 | 0.543 |
| 锁骨束腱膜长度 | 2.82±0.99 | 2.65±0.93 | 1.183 | 0.238 |
| 胸骨束腱膜长度 | 7.17±1.46 | 7.45±1.55 | -1.251 | 0.212 |
表5 不同性别健康志愿者胸锁乳突肌内部结构测量平均值(cm, |
| 项目 | 男性组 | 女性组 | t值 | P值 |
|---|---|---|---|---|
| 锁骨束止点宽度 | 3.27±0.67 | 2.89±0.70 | 3.740 | 0.000 |
| 锁骨束腱膜宽度 | 0.93±0.49 | 0.71±0.43 | 3.149 | 0.002 |
| 锁骨束腱膜厚度 | 0.09±0.04 | 0.08±0.03 | 1.331 | 0.185 |
| 胸骨束止点宽度 | 0.91±0.15 | 0.82±0.12 | 4.481 | 0.000 |
| 胸骨束腱膜宽度 | 0.78±0.25 | 0.64±0.20 | 4.102 | 0.000 |
| 胸骨束腱膜厚度 | 0.13±0.06 | 0.12±0.06 | 0.715 | 0.475 |
| 锁骨束腱膜长度 | 2.95±0.92 | 2.50±0.95 | 3.243 | 0.001 |
| 胸骨束腱膜长度 | 7.35±1.47 | 7.26±1.55 | 0.366 | 0.714 |
讨论
胸锁乳突肌为颈部重要肌肉,对头颈部直立姿势的维持起到重要作用。对于该肌肉的精细解剖结构,以往文献多限于描述其起止点,而对其内部结构少有报道[2, 3]。使用高频超声无创评价胸锁乳突肌的内部精细结构及有无变异,其意义有如下几点:(1)临床上胸锁乳突肌可发生的病变包括肌性斜颈、肌炎、肿瘤、结核、放疗相关纤维化等,如要准确诊断这些疾病并具体定位病变发生的位置,需要对胸锁乳突肌的正常内部超声表现有详细了解;(2)口腔颌面部手术有时会出现一些影响患者生活质量的并发症,如因术区组织缺损而导致的术后面部局部凹陷,因腮腺肿瘤切除术后腮腺副交感神经纤维与皮肤血管、汗腺的交感神经纤维发生交错连接而导致的味觉出汗综合征[4]等。已有许多临床研究[5, 6, 7, 8, 9]表明,胸锁乳突肌瓣可安全、有效地降低这些并发症的发生率,因此胸锁乳突肌瓣修补在口腔颌面部手术中的应用越来越广泛。术前使用超声检查患侧胸锁乳突肌各肌束厚度并观察有无解剖变异,有助于术前制定更详细的手术方案。
肌肉骨骼系统超声近10年来发展迅速,超声仪器成像质量的不断提升,也为高频超声清晰显示浅表肌肉内部结构提供了良好的硬件条件。
本研究中,横断面完整扫查可清晰显示胸锁乳突肌有无解剖学变异,共发现7例锁骨止点变异,均为单侧发生、2个锁骨头,该结果可能与样本量较小有关,如进行大规模正常人群筛查,理论上可能发现其他种类和数量的变异。
本研究的测值表明,双侧胸锁乳突肌对称,肌肉总厚度、各部分肌束厚度、其内部结构、止点处的双侧测值差异均无统计学意义(P均>0.05),故在该肌肉病变的发现及诊断中可以使用双侧对比的方法,增加诊断信心,提高准确率;受检者均为右利手,故肌肉厚度与优势手无关。本研究所得BMI与胸锁乳突肌总厚度及各部分厚度的相关分析中Pearson相关系数为0.286~0.371(P<0.01),表明BMI与肌肉厚度有弱相关性。
本研究的不足在于样本量较小且受检者均为中青年、右利手,无法进行年龄分层研究及左、右利手差异性的分析,未涉及胸锁乳突肌血供的观察和分析;故尚需扩大健康志愿者的样本量、年龄分布范围,并在后续的进一步研究中加入胸锁乳突肌血供的观察和分析。
综上所述,高频超声可有效显示胸锁乳突肌全程,并且可以定量描述其内部精细解剖结构及有无变异,为临床提供重要信息,助力胸锁乳突肌病变的诊断及使用胸锁乳突肌瓣的口腔颌面部手术的术前规划。