
乳腺化生性癌(metaplastic breast carcinoma,MBC)指乳腺腺上皮不同比例转化为另一种上皮组织或非腺上皮组织和(或)间叶组织[1]。MBC组织学类型多样,是一种罕见的乳腺恶性肿瘤,在所有乳腺恶性肿瘤中占比仅为0.2%~5.0%[2]。含有鳞状细胞癌成分的乳腺化生性癌(metaplastic carcinoma with squamous cell component,MCSC)更为少见,本研究中MCSC包括单纯性鳞状细胞癌、腺鳞癌、伴间叶分化的化生性癌和混合型化生性癌。既往关于MBC的报道多为小样本案例报道,对MCSC的研究更为少见,本文通过回顾性分析9例MCSC患者的超声声像图特征并与病理结果进行对比分析,以加深对此罕见肿瘤的认识,为超声诊断MCSC积累一定经验。
资料与方法
一、对象
回顾性分析2014年1月至2020年12月于湖北省肿瘤医院手术切除,经病理检查证实的9例MCSC患者,9例患者均因乳房肿块就诊,均为绝经期或围绝经期女性,年龄44~76岁,平均年龄(51.8±10.9)岁。9例均行乳腺癌改良根治术。所有MCSC患者术后均进行大体、镜下病理和免疫组化检查。
二、仪器与方法
2.免疫组化观察指标:免疫组化主要观察雌激素受体(estrogen receptor,ER)、孕激素受体(progesterone receptor,PR)和人表皮生长因子受体-2(human epidermal growth factor receptor-2,Her-2)的表达。
结果
一、超声表现
9例MCSC中,1例患者肿瘤为多发性,8例为单发性,其中左乳肿瘤3例,右乳肿瘤6例;外上象限肿瘤7例,乳房内侧肿瘤1例,1例为巨大肿瘤,直径约15 cm;肿瘤最大径1.07~15.00 cm,中位径线为4.48 cm;5例内部呈混合性回声,内均可见大小不等的不规则无回声区,4例内部呈低回声;9例后方回声均可见不同程度增强;7例边界欠清晰、浅分叶状或边缘模糊不清;8例形态不规则;3例伴多发性密集簇状钙化;超声检查有4例患者腋下淋巴结肿大,其中3例经病理证实为淋巴结转移。CDFI显示肿瘤实性部分血流较丰富,Adler血流分级:8例为Ⅲ级,1例为I级。BI-RADS分级:5例5类,3例4c类,1例4b类,超声诊断恶性肿瘤符合率100%(表1)。
表1 9例MCSC的超声表现与病理结果 |
| 病例序号 | 年龄(岁) | 肿瘤位置 | 肿瘤最大径线(cm) | 内部回声 | Adler血流分级 | 后方回声增强 | 钙化 | BI-RADS分级 | 腋下淋巴结肿大 | 病理分型 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 51 | 右乳、外上 | 4.12 | 实质性 | Ⅲ | 有 | 有 | 5 | 有 | 混合型化生性癌 |
| 2 | 57 | 左乳、外上 | 4.04 | 囊实性 | Ⅲ | 有 | 无 | 4c | 有 | SCC |
| 3 | 47 | 右乳、外上 | 2.78 | 实质性 | I | 有 | 有 | 5 | 无 | ASC |
| 4 | 47 | 右乳内侧 | 1.07 | 实质性 | Ⅲ | 有 | 无 | 4b | 无 | SCC |
| 5 | 44 | 右乳 | 15.00 | 囊实性 | Ⅲ | 有 | 无 | 5 | 有 | 混合型化生性癌 |
| 6 | 45 | 左乳、外上 | 2.74 | 实质性 | Ⅲ | 有 | 无 | 4c | 有 | 混合型化生性癌 |
| 7 | 79 | 右乳、外上 | 3.54 | 囊实性 | Ⅲ | 有 | 有 | 5 | 无 | 混合型化生性癌 |
| 8 | 46 | 右乳、外上 | 2.95 | 实质性 | Ⅲ | 有 | 无 | 5 | 无 | SCC |
| 9 | 51 | 左乳、外上 | 4.09 | 囊实性 | Ⅲ | 有 | 无 | 4c | 无 | 伴间叶分化的化生性癌 |
注:MCSC为含有鳞状细胞癌成分的乳腺化生性癌;SCC为单纯性鳞状细胞癌;ASC为腺鳞癌;BI-RADS为乳腺影像报告与数据系统 |
二、病理结果
病理诊断乳腺鳞状细胞癌3例,腺鳞癌1例,伴间叶分化的化生性癌1例(癌为高级别浸润性导管癌、导管原位癌及鳞状细胞癌,间叶成分为软骨肉瘤、多形性平滑肌肉瘤),混合型化生性癌4例(1例伴大汗腺分化癌)。
{kind=link}
{kind=link}
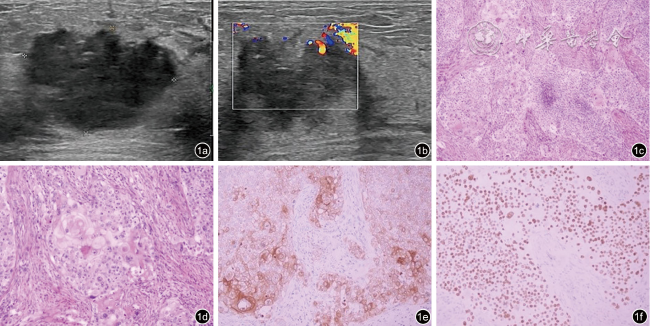
图1 含鳞状细胞癌成分的乳腺化生性癌的超声及病理图像(病例8)。图a为超声图像示肿块呈低回声,边界模糊形态不规则,未显示明显钙化;图b为彩色多普勒图像示肿块血流信号增多;图c为病理图像示肿瘤呈实性片状伴局部坏死,无腺管形成,可见角化珠和细胞间桥(HE ×100);图d为病理图像示肿瘤细胞核深染,核浆比增大,胞浆嗜酸,核分裂象可见(HE ×200);图e为免疫组织化学图像示肿瘤细胞CK5/6胞质阳性(EnVision法×200);图f为免疫组织化学图像示肿瘤细胞P40胞核弥漫强阳性(EnVision法 ×200) |
表2 9例MCSC的病理分型与腋窝淋巴结转移情况 |
| 病例序号 | 年龄(岁) | 病理分型 | 腋窝淋巴结转移 | 免疫组化 |
|---|---|---|---|---|
| 1 | 51 | 混合型化生性癌 | 腺癌(4/19枚) | ER(-)PR(-)Her-2(浸润性导管癌部分3+,鳞癌部分1+) |
| 2 | 57 | SCC | 无 | ER(10%,2+)PR(2%,2+)Her-2(-) |
| 3 | 47 | ASC | 无 | ER(1+,1%)PR(-)Her-2(-) |
| 4 | 47 | SCC | 无 | ER(-)PR(-)Her-2(2+) |
| 5 | 44 | 混合型化生性癌 | 鳞状细胞癌(1/14枚),腺癌(10/14枚) | ER(5%,2+)PR(2%,1+)Her-2(3+) |
| 6 | 45 | 混合型化生性癌 | 腺癌(2/21枚) | ER(-)PR(-)Her-2(-) |
| 7 | 79 | 混合型化生性癌 | 无 | ER(-)PR(-)Her-2(-) |
| 8 | 46 | SCC | 无 | ER(-)PR(-)Her-2(-) |
| 9 | 51 | 伴间叶分化的化生性癌 | 无 | ER(-)PR(-)Her-2(1+) |
注:MCSC为含有鳞状细胞癌成分的乳腺化生性癌;SCC为单纯性鳞状细胞癌;ASC为腺鳞癌;ER为雌激素受体;PR为孕激素受体;Her-2为人表皮生长因子受体-2 |
讨论
MBC与非特殊类型浸润性癌相比具有较高的侵袭性和复发率,预后差。由于乳腺MBC成分构成不同,影像学表现并没有特异性,较难与其他类型的乳腺恶性肿瘤相鉴别,有时甚至表现出良性特征[5]。大部分MBC是三阴性乳腺癌[6],内分泌治疗效果较差,因此对于MBC早发现早治疗至关重要。本研究中9例MCSC患者,发病年龄44~76岁,中位年龄51.8岁,肿块最大径1.07~15.00 cm,中位径线4.48 cm。与既往文献报道所认为的乳腺MBC的发病年龄多为中老年,就诊时乳腺肿瘤体积较大一致[7-8]。Rakha等[9]认为东方人乳腺MBC中以鳞状细胞癌最常见,而本研究中MCSC以混合型化生性癌最多(4/9),其次是鳞状细胞癌(3/9)。
本研究9例MCSC中超声检查5例可见大小不等的不规则无回声暗区,超声所见的不规则暗区与大体标本出血坏死囊性区的表现相吻合。镜下囊性区域可见鳞状细胞癌原发灶中心细胞聚集,囊壁可见典型鳞状细胞癌结构,伴坏死及囊腔形成。含有鳞状细胞癌成分的肿瘤生长迅速,内部供血不足导致瘤体内部发生囊性变,鳞状细胞癌由囊壁脱落坏死形成腔隙。本研究观察到9例患者的肿瘤后方回声均呈不同程度的增强,考虑与其内部存在囊性成分有关[10];这一表现与多数乳腺浸润性导管癌肿块后方回声衰减明显不同。本研究9例中8例可见大小不等的囊性病变,病理分型中鳞状细胞癌成分所占比例较高(60%~100%),仅1例MCSC的大体标本切开未见囊性病变,该例病理结果为(左乳)混合型化生性癌(浸润性微乳头状癌约60%,浸润性导管癌Ⅲ级成分约40%,局灶呈化生性癌改变,化生性癌成分为鳞状细胞癌)伴间质淋巴细胞浸润。该肿瘤超声表现为实质性肿瘤,可能与鳞状细胞癌含量较少,癌成分较复杂有关。
9例患者的其他超声表现为:边界欠清晰或边缘模糊(7/9)、形态不规则(8/9)、3例均表现为多发性密集簇状钙化(3/9)、CDFI显示病灶实性部分血流较丰富,Adler血流信号分级大多为Ⅲ级(8/9),以上表现均符合乳腺恶性肿瘤的声像图特点。根据乳房肿瘤的以上特征,本研究中BI-RADS分级1例分为4b类,其余均为4c~5类,术前超声将乳腺肿瘤均分类为几乎确定的恶性肿瘤,超声诊断恶性肿瘤与病理结果符合率为100%。
综上所述,MCSC的超声表现为恶性肿瘤的声像图特征。肿瘤体积较大、瘤体内部为混合性回声伴后方回声增强、肿瘤实质部分血供丰富的超声表现对诊断MCSC有意义。但本研究病例数少,病理学亚型有限,今后将加大样本量进一步探讨。