
20世纪80年代,McGoon指数(McGoon index,MGI)和肺动脉指数(pulmonary artery index,PAI)又称Nakata指数开始用于评估先天性心脏病(congenital heart disease,CHD)患者的肺血管发育[1-2],MGI被认为是评价肺血管床整体发育的指标。临床上,MGI常与Nakata指数共同作为法洛四联症(tetralogy of Fallot,TOF)一期根治手术最重要的手术指征,在TOF患者术前评估、术式选择及术后干预方面提供了重要的参考依据,与患者预后密切相关[3]。Hiraishi等[4]应用心血管造影与超声心动图分别测量主肺动脉(main pulmonary artery,MPA)、右肺动脉(right pulmonary artery,RPA)、左肺动脉(left pulmonary artery,LPA)的近端、中端、远端内径以及肺动脉狭窄处内径,发现超声与心血管造影测值高度相关,提示超声测量的MGI可以较准确地评估肺动脉的发育程度,指导手术方式的选择。过去MGI主要用于成人或儿童CHD患者的评估,但胎儿时期血流动力学及肺发育情况与出生后截然不同,近些年已有对胎儿MGI的研究报道。郭勇等[5]对TOF胎儿的研究显示,MGI明显低于正常胎儿,提示此类CHD在胎儿时期可能已经对肺动脉发育产生一定不良影响。同时发现RPA和LPA内径之和与胎儿肺体积呈明显的线性正相关,提示二维超声测量左右肺动脉一定程度上可反映胎儿肺发育情况。本文将进一步探讨不同孕龄正常胎儿的MGI变化情况及在不同肺血流量状态下的多种类型CHD胎儿MGI的差异,并探索其临床应用价值。
资料与方法
一、对象
回顾性选取2020年6月至2021年8月在浙江大学医学院附属邵逸夫医院超声科接受超声心动图检查的胎儿,根据胎儿超声心动图检查规范[6]进行系统全面扫查选取未见明显异常的218例胎儿作为正常组,孕妇年龄20~40岁,孕龄18~33+6周。根据孕龄不同,再将正常组分为4个亚组,孕18~21+6周22例;孕22~25+6周64例;孕26~29+6周105例;孕30~33+6周27例。连续选取同时期胎儿超声心动图诊断包含“肺动脉狭窄”或“肺动脉闭锁”等考虑肺动脉血流减少或闭锁的CHD胎儿66例为病例组1,孕妇年龄21~38岁,孕龄18~32周;选取超声心动图诊断包含“主动脉狭窄”“主动脉缩窄“或“主动脉弓离断”等考虑主动脉血流减少或离断胎儿19例为病例组2,孕妇年龄26~41岁,孕龄20~33周。排除标准:(1)无法清楚显示左、右肺动脉分支或膈肌水平降主动脉;(2)肺动脉闭锁合并室间隔缺损(pulmonary atresia with ventricular septal defect,PA/VSD)Boston分型中的Ⅳ型,无法显示LPA及RPA;(3)合并膈疝等心外畸形、肺部疾病、心肌病、羊水过少或多胎妊娠等可能影响胎儿肺或肺血管发育的情况。本研究所有孕妇均签署胎儿超声心动图检查知情同意书。本研究经浙江大学医学院附属邵逸夫医院伦理委员会批准(批件号:20200210-78)。
二、仪器与方法
1. 仪器:采用Philips EPIQ7C彩色多普勒超声诊断仪,探头选用S5-1和S8-3,频率分别为1~5 MHz和3~8 MHz。
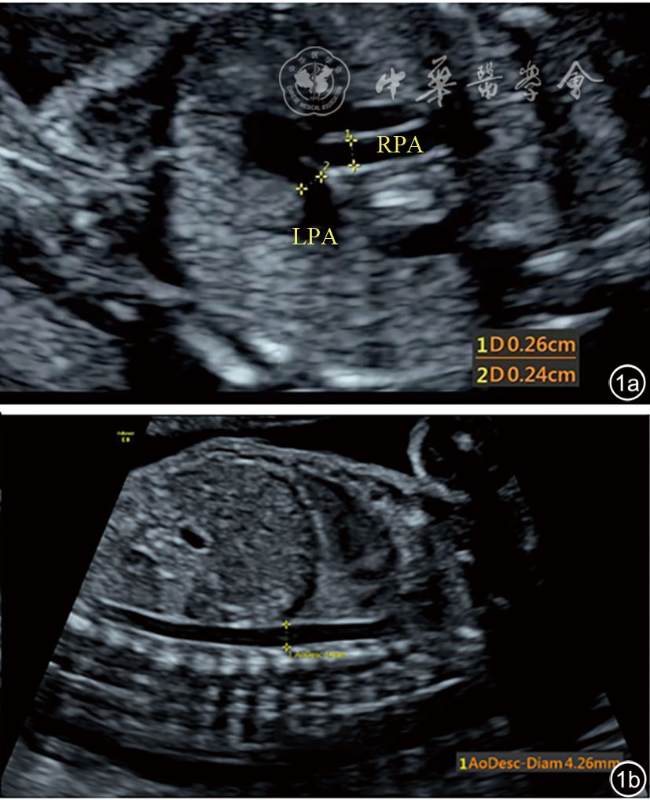
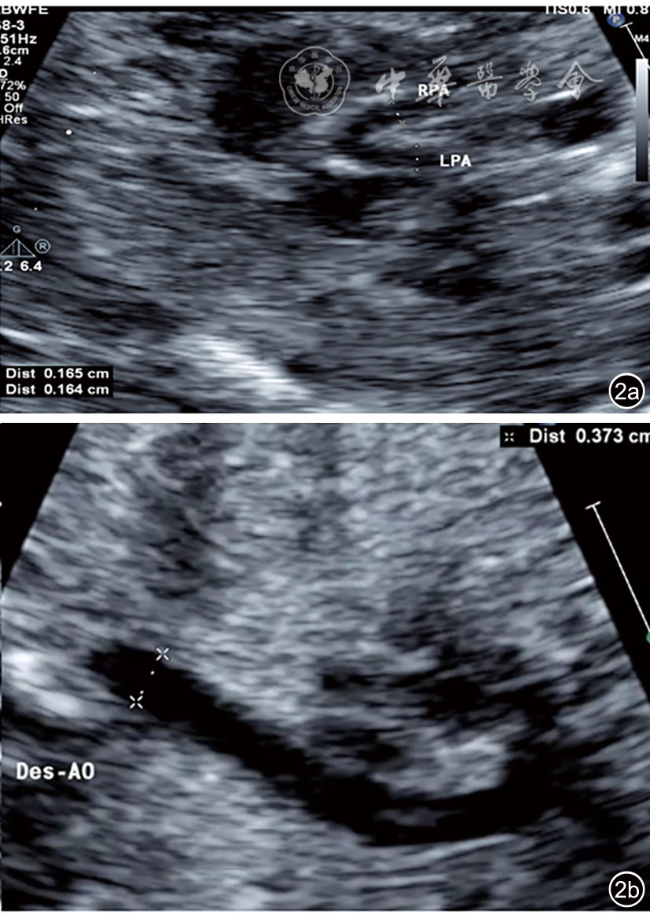
2.胎儿超声心动图检查:(1)胎儿生物学指标测量,确定孕龄;(2)测量并计算胎儿心胸比(cardiothoracic ratio,CTR);(3)收缩期测量胎儿主动脉瓣环(aorta,AO)内径及肺动脉瓣环(pulmonary,PA)内径,计算PA/AO;(4)胎儿MGI的测定:留存清晰显示LPA、RPA、膈肌水平降主动脉(descending aorta,DAO)、动脉导管(ductus arteriosus,DA)的动态图。测量LPA、RPA、DAO、DA内径,所有数值均在心室收缩期完成[7](图1,2),至少测量3次,取平均值。计算MGI公式为:(LPA内径+RPA内径)/膈肌水平DAO内径。所有图像采集均由同一名具有10年以上胎儿超声心动图经验的高年资医师完成。图像的后期测量及运算均由另一位具有3年以上胎儿超声心动图经验的医师完成。
三、统计学分析
应用SPSS 23.0软件进行统计学分析,计量资料以 表示,所有资料经正态性检验及方差齐性检验,正常对照组内4个亚组之间的比较及正常对照组与病例组间的比较均采用单因素方差分析,进一步多重比较分析采用LSD-t法。以P<0.05为差异有统计学意义。
表示,所有资料经正态性检验及方差齐性检验,正常对照组内4个亚组之间的比较及正常对照组与病例组间的比较均采用单因素方差分析,进一步多重比较分析采用LSD-t法。以P<0.05为差异有统计学意义。
表示,所有资料经正态性检验及方差齐性检验,正常对照组内4个亚组之间的比较及正常对照组与病例组间的比较均采用单因素方差分析,进一步多重比较分析采用LSD-t法。以P<0.05为差异有统计学意义。结果
一、正常对照组4个不同孕龄的亚组间MGI比较
正常对照组(18~21+6周)共22例,MGI为1.39±0.35(0.95~2.31);正常对照组(22~25+6周)共64例,MGI为1.38±0.20(0.92~1.97);正常对照组(26~29+6周)共105例,MGI为1.38±0.21(0.94~1.87);正常对照组(30~33+6周)共27例,MGI为1.40±0.19(1.10~1.87),4组之间MGI比较差异均无统计学意义(P>0.05),提示中晚孕期正常胎儿MGI相对稳定,不随孕龄增加而改变。
二、正常对照组与病例组间超声心动图参数比较
正常对照组共218例,CTR为0.25±0.04,PA/AO为1.278±0.133,MGI为1.38±0.22;病例组1共66例,CTR为0.28±0.05,PA/AO为0.745±0.276,MGI为1.16±0.19;病例组2共19例,CTR为0.26±0.03,PA/AO为1.302±0.746,MGI为1.42±0.25。病例组1的CTR大于正常组,差异有统计学意义(P<0.05)。病例组1的MGI低于其他2组,差异有统计学意义(P<0.05),病例组2的MGI高于病例组1,差异有统计学意义(P<0.05),而和正常对照组比较差异无统计学意义(P>0.05,表1)。
表1 正常对照组与病例组各组间超声心动图参数比较( |
 )
){kind=link}
{kind=link}
{kind=link}
{kind=link}
| 组别 | 例数 | H/C | PA/AO | MGI |
|---|---|---|---|---|
| 正常对照组 | 218 | 0.25±0.04 | 1.278±0.133 | 1.38±0.22 |
| 肺动脉血流减少或闭锁组 | 66 | 0.28±0.05a | 0.745±0.276ab | 1.16±0.19ab |
| 主动脉血流减少或离断组 | 19 | 0.26±0.03 | 1.302±0.746 | 1.42±0.25 |
| F值 | 7.79 | 117.8 | 27.78 | |
| P值 | <0.01 | <0.01 | <0.01 |
注:H/C为心胸比;PA/AO为肺动脉与主动脉内径比值;MGI为McGoon指数;与正常对照组比较,aP<0.05;与主动脉血流减少或离断组比较,bP<0.05 |
三、随访情况
病例组1的66例CHD胎儿中,有8例胎儿在不同孕龄进行复查,故孕妇的例数仅为58例,其中14例失访,失访率24.1%,25例引产,19例出生。出生的19例中,1例出生后情况差,无法耐受手术,放弃治疗后死亡(孕22周时MGI为1.37);1例出生后行TOF姑息治疗手术,术后多器官衰竭死亡(孕24周时MGI为1.20);3例(MGI 1.05~1.22)需择期进行TOF根治术;5例(MGI 0.88~1.35)出生后紧急或择期进行经皮球囊肺瓣狭窄成形术;9例(MGI 0.89~1.64)出生后情况良好,门诊随访,无需手术干预。
讨论
严重肺动脉狭窄(pulmonary stenosis,PS)胎儿出生后心血管结构及功能状态复杂多变,需根据每个患儿的肺动脉发育情况制定个体化的治疗策略[8]。Nakata等[1]研究发现,在肺动脉发育不全的患者中,手术死亡和心力衰竭的发生率更高。肺血管发育情况是PS最重要的手术参考指征,其与术后转归密切相关,MGI被用于评估CHD患者肺血管床整体生长情况,低MGI提示肺发育不全,并与预后不良相关[2,9]。MGI广泛应用于出生后儿童及成人CHD中,可以通过心血管造影、CT、超声心动图等检查获得[10,11,12,13]。多位学者在关于先天性膈疝(congenital diaphragmatic hernia,CDH)患儿的研究中表明,MGI可用来评估肺血管的发育情况,结果显示MGI与肺血管发育呈正相关,可作为评估CDH患儿预后和死亡率的预测因子[14,15,16]。另有学者发现MGI用于评价肺血管发育,是TOF患者手术风险预测或术后随访中的主要参数[17,18,19]。
MGI广泛应用于出生后儿童及成人中并不断有研究证实其应用价值,但是由于胎儿时期血流动力学及肺发育情况与出生后截然不同,MGI应用于胎儿时期的价值有待探索。Guo等[20]研究110例21.3~31.5周正常胎儿的MGI为1.30±0.179(0.94~1.93);54例21.4~34.4周肺血流量减少型CHD胎儿的MGI为1.146±0.216(0.33~1.58)。张烨等[21]对100例19~36周正常胎儿的研究显示MGI为1.31±0.35。本研究对218例孕龄为18~33+6周正常胎儿的研究结果显示中晚孕期正常胎儿的MGI为1.38±0.22,与既往研究结果基本一致。但本研究不同于既往研究的是,本研究采集的正常胎儿样本量孕龄覆盖范围广,并按照孕龄分为4组,结果显示各孕龄胎儿的MGI无明显差异,说明MGI不随孕龄改变而改变。分析原因为MGI为LPA和RPA内径之和与DAO的比值,反映了胎儿肺动脉与主动脉发育过程中的相对比例关系,而诸多研究已证实肺动脉与主动脉发育均随孕龄增加而增长[22,23,24,25,26],因此在正常发育的胎儿中,MGI不会随孕龄的增加而增大,而是相对稳定地保持在一定的正常范围内。
与儿童CHD患者的研究结果一致[3-4,7,8,9,10],本研究对肺动脉血流减少或闭锁的66例CHD胎儿研究显示,其MGI明显小于正常胎儿,提示这类CHD已经对胎儿肺血管发育造成一定影响,同时其CTR明显大于正常胎儿,可能由于肺血流减少型CHD影响胎儿肺的发育导致肺体积相对小,继而导致心胸面积比值增大。而同时对主动脉血流量减少或离断的19例胎儿研究提示,其MGI明显大于肺血流量减少或闭锁组,且与正常对照组无显著差异,这也证明了MGI能够较准确反映肺动脉的血流量变化,因此MGI可以作为诊断或鉴别诊断肺动脉狭窄的有效参数。本研究及既往对CHD胎儿的研究[20-21]均提示胎儿MGI能够在产前评价胎儿肺动脉发育情况,这对于动态评估宫内进展型CHD胎儿的心血管发育、指导病情及预后分析、提供产前合理咨询信息具有重要价值。目前用于产前评价胎儿心血管结构与血流动力学的主要技术仍然是胎儿超声心动图,尽管MRI已经用于胎儿颅脑、脊柱等部位的产前结构评估,但在胎儿心血管畸形诊断方面的应用还非常有限。胎儿超声心动图测量MGI需要获取清晰的LPA、RPA、DAO图像以保证测量的准确性,本研究的切面获取均由经验丰富的高年资医师完成,定量LPA、RPA、DAO内径则通过至少3次测量取平均值,保证了本研究MGI测量的可重复性和准确性。
本研究尚存在一定局限性:(1)早孕期胎儿MGI难以测量,故未纳入进行研究。(2)本研究未对胎儿出生前以及出生后肺血管及肺发育进行系统的随访研究,纵向追踪产前、产后MGI的变化必然更有助于对不同肺血流状态下胎儿、新生儿及幼儿肺血管的发育情况进行全面系统评估。
综上所述,孕18~33+6周阶段胎儿MGI不随孕龄的增加而改变,超声心动图定量测量胎儿MGI可评价不同CHD胎儿的肺血流量,一定程度上反映肺血管发育情况。