
Duchenne肌营养不良(Duchenne muscular dystrophy,DMD)是进行性肌营养不良中最常见的一种类型[1],发病率约为1/3500。病因为基因片段缺失导致基因编码抗肌萎缩蛋白缺失[2-3],进而发生肌纤维坏死、纤维化及再生能力的丧失,临床上主要表现为进行性骨骼肌退化和心脏、膈肌功能障碍[4-5]。患者多在20岁前死于呼吸衰竭或心力衰竭[6-7]。目前DMD患者的康复治疗以控制病情进展为目标,在终生治疗过程中,呼吸功能评估是明确病情进展的重要环节。国外专家共识认为,对于认知受损且无法可靠地进行呼吸功能测试的患儿,应培训使用辅助装置[8]。文献显示,患者呼吸衰竭主要是因为膈肌受累[5,9]。超声可准确评估膈肌移动度(diaphragmatic excursion,DE)、膈肌增厚率(diaphragm thickening fraction,DTF),而DE和DTF与呼吸功能变化呈显著正相关[10-11]。目前,超声评价DMD患儿膈肌功能的研究鲜见报道,因此,本研究拟通过超声准确测量右锁骨中线、右侧腋前线DE及DTF,从而评估DMD患儿的膈肌运动功能。
资料与方法
一、对象
收集2021年5月1日至2022年3月1日,在解放军总医院第三医学中心接受治疗的DMD患儿21例,均为男性,年龄3~15岁,平均年龄(8.4±3.0)岁。纳入标准:(1)行动困难、双侧腓肠肌假性肥大等临床表型已诊断;(2)已通过分子诊断技术明确诊断。排除标准:(1)临床诊断其他类型肌营养不良;(2)其他原因引起的继发性肢体肥大;(3)中途退出研究及数据不完整。同期纳入同年龄段的健康儿童志愿者21例为对照组,均为男性,平均年龄(8.8±3.2)岁。本研究是一项前瞻性研究,获得解放军总医院伦理委员会的批准(批件号:S2022-165-01),研究取得家属或监护人的知情同意,并签署知情同意书。
二、仪器与方法
1.仪器:使用Philips iE Elite彩色多普勒超声诊断仪,选用C5-1凸阵探头、L11-3线阵探头,频率分别为1~5 MHz、3~11 MHz。
2.膈肌超声检查:患儿取平卧位,于平静呼吸状态下检查。由于以脾脏作为声窗测量左半膈肌运动相对困难,目前超声评估膈肌运动时常以肝脏作为声窗测量右半膈肌。将探头置于右侧锁骨中线第8~10肋间隙,使超声束与膈肌垂直,二维超声图像上显示3层平行的组织结构,包括两条高回声的胸膜层和腹膜层以及中间低回声的肌肉层;膈肌的厚度(diaphragm thickness,Tdi)为胸膜层与腹膜层之间的距离;在二维超声定位膈肌后,使用M型超声观察膈肌运动,膈肌运动幅度至少测量3个呼吸周期,取平均值。
3.观察指标:(1)DE测量:使用凸阵探头测量DE,在M型超声图像上,将采样线垂直于膈肌,以胸膜高回声线为标志,记录波峰与波谷之间的距离,即为DE,DE=膈肌吸气末高度与膈肌呼气末高度的差值(图1)。(2)DTF测量:使用线阵探头测量DTF。在二维超声图像上定位膈肌位置,切换M型模式,使取样线与膈肌垂直,分别测量取样线上吸气末与呼气末Tdi,以获取DTF,DTF=(吸气末Tdi-呼气末Tdi)/呼气末Tdi×100%。同样的方法,将探头置于右侧腋前线肋缘下,获取DE及DTF。

4.病理组织检查和实验室检查:DMD病例组均进行病理组织检查和实验室检查。(1)单侧肱二头肌病理组织活检,常规石蜡包埋,行苏木精-伊红(hematoxylin eosin,HE)染色,光镜下观察病理变化,并进行基因检测。(2)实验室检查:行血清肌酸激酶(creatine kinase,CK)水平检测。
三、统计学分析
采用SPSS 22.0医学统计软件进行数据分析,符合正态分布的计量资料以 表示。采用独立样本t检验比较DMD组与健康儿童组2组数据的组间差异,同一组内吸气末Tdi与呼气末Tdi比较采用配对t检验。以P<0.05为差异有统计学意义
表示。采用独立样本t检验比较DMD组与健康儿童组2组数据的组间差异,同一组内吸气末Tdi与呼气末Tdi比较采用配对t检验。以P<0.05为差异有统计学意义
表示。采用独立样本t检验比较DMD组与健康儿童组2组数据的组间差异,同一组内吸气末Tdi与呼气末Tdi比较采用配对t检验。以P<0.05为差异有统计学意义结果
一、一般资料
(一)临床表现
病例组DMD患儿21例,临床主要表现为双侧腓肠肌假性肥大,其中10例(3~8岁)肢体活动能力较同龄人减低,走、跳等行动困难,11例(9~15岁)患儿依靠轮椅出行。同期对照组21例健康儿童志愿者,发育正常,行动灵活无障碍。2组年龄比较,差异无统计学意义(t=0.800,P=0.692)。
(二)病理组织检查和实验室检查结果
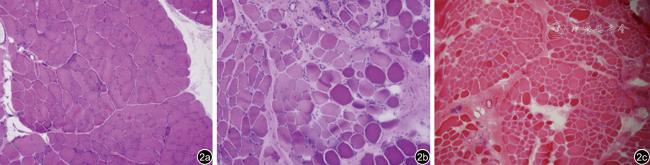
肱二头肌病理组织HE染色见肌纤维大小显著不等,少量坏死纤维及再生肌纤维,肌内膜及肌束膜中、重度增生(图2);基因检测显示外显子缺失或重复。实验室血清CK为(9316.2±5704.9)U/L,明显高于正常值(18~198) U/L。
二、超声表现
(一)二维超声表现
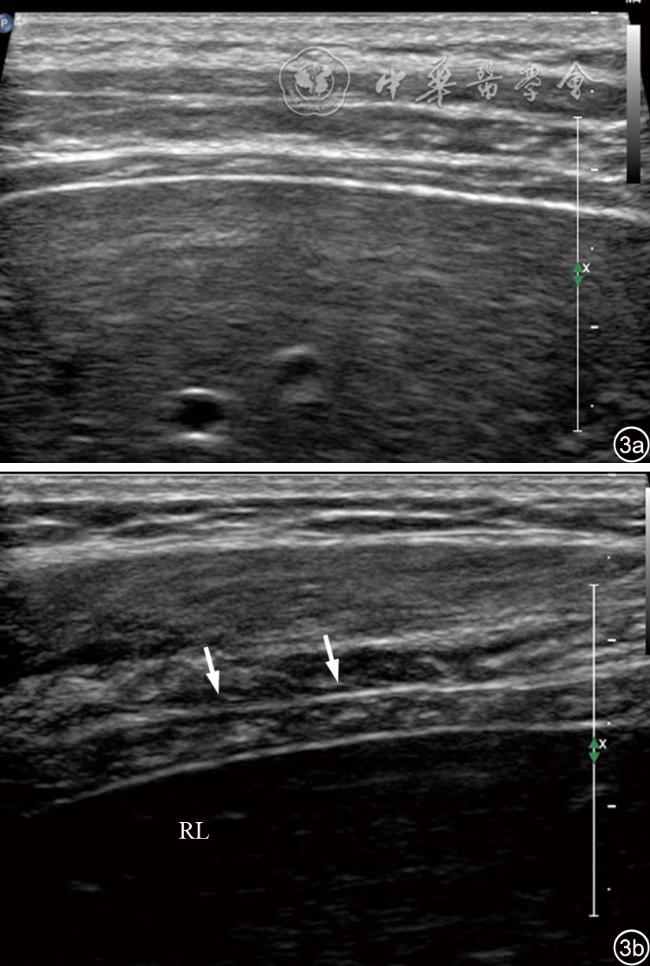
健康儿童膈肌表现为均匀的低回声,中间可见结缔组织形成的条带状高回声线,与胸膜线、腹膜线走行较一致。与正常对照组比较,DMD组右侧腋前线和锁骨中线2个切面呼气末Tdi与吸气末Tdi明显增厚(P均<0.001),膈肌回声增强、不均匀,肌肉间结缔组织形成的条带状高回声线部分消失或减低,正常膈肌结构紊乱或消失(图3)。
(二)M型超声表现
1. DMD组、正常对照组吸气末Tdi与呼气末Tdi比较:DMD组右侧腋前线吸气末Tdi(4.26±0.60)mm、呼气末Tdi(4.05±0.59)mm,右侧锁骨中线吸气末Tdi(4.62±0.60)mm,呼气末Tdi(4.35±0.59)mm,两切面Tdi随呼吸周期均无明显变化(P=0.593、0.493);而对照组21例健康儿童,右侧腋前线吸气末Tdi(1.72±0.24)mm、呼气末Tdi(0.18±0.21)mm,右侧锁骨中线吸气末Tdi(1.69±0.30)mm、呼气末Tdi(0.99±0.20)mm,两切面Tdi随呼吸周期变化显著(P=0.004、0.006,表1)。
表1 DMD组、正常对照组膈肌吸气末厚度与呼气末厚度比较(mm, |
 )
)| 组别 | 例数 | 右侧腋前线 | t值 | P值 | 右侧锁骨中线 | t值 | P值 | ||
|---|---|---|---|---|---|---|---|---|---|
| 吸气末Tdi | 呼气末Tdi | 吸气末Tdi | 呼气末Tdi | ||||||
| DMD组 | 21 | 4.26±0.60 | 4.05±0.59 | 0.874 | 0.593 | 4.62±0.60 | 4.35±0.59 | 0.913 | 0.493 |
| 对照组 | 21 | 1.72±0.24 | 1.18±0.21 | 0.841 | 0.004 | 1.69±0.30 | 0.99±0.20 | 0.527 | 0.006 |
注:DMD为Duchenne肌营养不良;Tdi为膈肌厚度 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
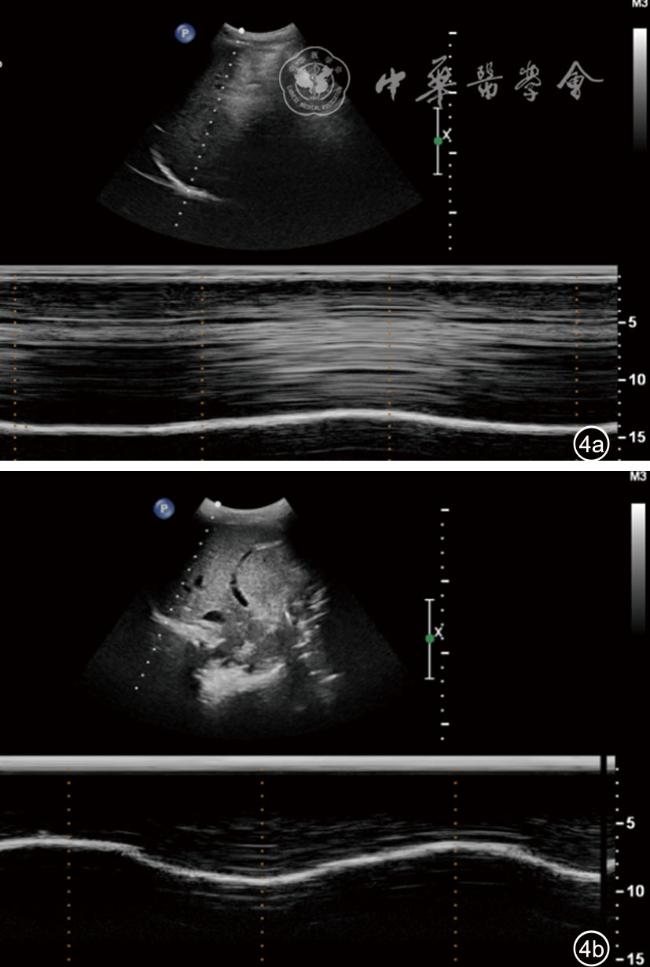
图4 右侧腋前线切面Duchenne肌营养不良患儿与正常儿童膈肌超声图像。图a示Duchenne肌营养不良患儿膈肌运动幅度随呼吸运动变化减弱,接近平直,吸气末与呼气末膈肌的厚度未见明显变化;图b示正常儿童膈肌随呼吸运动变化明显,呈“大波浪”样表现 |
表2 DMD组与正常对照组DE、DTF对比 |
| 组别 | 例数 | 右侧锁骨中线DTF(%) | 右侧腋前线DTF(%) | 右侧锁骨中线DE(mm) | 右侧腋前线DE(mm) |
|---|---|---|---|---|---|
| DMD组 | 21 | 32.9±19.0 | 38.3±19.4 | 11.7±4.1 | 12.0±5.0 |
| 对照组 | 21 | 49.7±11.5 | 50.6±10.9 | 20.0±5.3 | 19.0±3.3 |
| t值 | 0.079 | 0.013 | 0.603 | 0.207 | |
| P值 | 0.002 | 0.015 | <0.001 | <0.001 |
注:DMD为Duchenne肌营养不良;DTF为膈肌增厚率;DE为膈肌移动度 |
讨论
此外,DMD患儿膈肌运动幅度随着呼吸运动变化明显减弱,甚至部分接近平直,右侧腋前线及右侧锁骨中线DE均较正常对照组减低,与对照组健康儿童膈肌“大波浪”运动的超声表现存在明显差异,这也进一步反映了DMD患儿呼吸期间膈肌收缩能力明显下降。
本研究尚存在一些不足之处:纳入样本量偏少,均为男性。原因在于DMD为罕见病,且该病为X连锁隐性遗传性肌肉变性疾病,发病主要为男性患者,女性携带者大多表型正常。因此,期望在后期建立病例库,进行进一步病例积累和研究探讨。
综上所述,超声具有无创、实时、可重复检测的优势,可有效评价DMD患儿膈肌功能,定量测量膈肌DTF、DE有助于DMD患儿病情监测。