
乳腺癌是女性发病率最高的恶性肿瘤[1]。乳腺癌患者在接受系统治疗后仍有3%~15%的复发风险,而复发是导致乳腺癌患者死亡的主要原因[2]。当前,我国乳腺癌患者基数大,所有的患者在治疗后均需长期随访,不仅增加了社会的医疗负担,还会导致患者家庭的经济压力。目前,乳腺癌术后随访方案对所有患者基本统一,并未考虑个人的复发风险。通过预测患者的术后复发风险,可帮助医师制定个性化随访方案,避免不必要的随访产生额外费用以及假阳性对患者造成的心理压力[3]。乳腺癌具有高度异质性,不同分子分型预后差异大,其中Luminal B 型是最常见的分子分型,占各分子分型的40%[4],研究显示,Luminal B 型的复发风险显著高于Luminal A 型,尤其是在确诊后5年内[风险比(hazard ratio,HR)=2.86],而5 年后的晚期复发风险相对较低(HR=0.65)[5,6],因此预测Luminal B 型乳腺癌患者术后5 年内的复发风险至关重要。以往评估术后复发风险是通过临床病理因素(如肿瘤大小、淋巴结状态、组织学分级等)对患者进行风险分组,但这种方法的中、高危复发风险组可变性大,无法指导个性化治疗与随访[7]。多基因检测工具可相对准确地评估早期乳腺癌患者的复发风险等级,但其是一种昂贵的侵入性方法,适用人群较局限[8]。针对Luminal B 型乳腺癌患者建立复发风险预测模型,以经济、无创、准确的方法指导个性化治疗及随访具有重要的临床价值。
在我国,手持超声是乳腺癌筛查和检查的首选方法。自动乳腺超声(automated breast ultrasound,ABUS)是乳腺三维超声成像技术,ABUS 技术的出现弥补了手持超声操作者依赖性强和无法标准化成像的不足,并且其具有扫诊分离的特点,可减轻超声医师的工作压力,实现高效、高质量的筛查与检查[9]。此外,ABUS 显示的冠状切面已被证明可提高诊断准确性,且可更好地显示病灶的边缘以及评估病灶范围,有利于医师进行术前评估[10,11]。经文献检索,目前尚无基于ABUS 图像预测乳腺癌复发风险的相关研究。因此,本研究基于术前ABUS 图像联合临床病理特征建立Luminal B 型乳腺癌患者术后复发风险的预测模型,并探讨模型的临床价值。
资料与方法
一、对象
收集2016 年1 月至2019 年12 月期间于西京医院确诊并接受乳腺癌手术治疗的浸润性乳腺癌女性患者,随访截止时间为2024 年9 月。纳入标准:(1)经病理证实为浸润性乳腺癌并且免疫组化结果为Luminal B 型;(2)初发的单侧乳腺癌;(3)具有完整的临床病理资料;(4)手术前行ABUS 检查。排除标准:(1)ABUS 检查前行新辅助治疗;(2)术前已发生远处转移;(3)既往有乳腺癌病史或合并其他恶性肿瘤史;(4)多发病灶;(5)失访。本研究为回顾性研究,经空军军医大学附属西京医院伦理委员会审批通过(批件号:KY20192119-F-1),经审批不需患者签署书面知情同意。
二、方法
1.随访与终点:本研究将复发定义为局部区域复发[局限于同侧乳腺或胸壁和(或)腋窝、锁骨上下及内乳淋巴结]或远处转移。为监测术后复发情况,所有患者术后每年至少有一次随访记录,通过影像学方法实施监测,使用病理学检查对可疑病灶进行确诊。本研究终点为无复发生存期(recurrence-free survival,RFS),定义为患者手术之日至出现复发事件日期或本研究随访截止日期。
2.临床病理特征:通过查阅电子病历获取患者的临床和病理信息,包括发病年龄(<45 岁、≥45 岁)、绝经情况(绝经、未绝经)、手术治疗方式(保乳术、全乳切除术)、新辅助化疗(是、否)、化疗(是、否)、放疗(是、否)、孕激素受体(progesterone receptor,PR)状态(阴性、阳性)、人表皮生长因子受体2(human epidermal growth factor receptor 2,HER2)状态(阴性、阳性)、Ki-67 表达(<30%、≥30%)、病理T 分期(T1、T2、T3)、病理N 分期(N0、N1、N2、N3)、组织学分级(Ⅰ/Ⅱ级、Ⅲ级)。在治疗方面,所有患者均按照国内外乳腺癌诊治指南推荐的治疗方案进行规范化治疗[7,12]。PR 状态,免疫组化结果“-”定义为阴性,“1+”“2+”“3+”定义为阳性;HER2 状态,免疫组化结果为“3+”定义为阳性,“-”“1+”定义为阴性,如果结果为“2+”,根据荧光原位杂交(fluorescence in situ hybridization,FISH)扩增结果确定HER2 状态,即有FISH 扩增HER2 为阳性,无FISH 扩增HER2 为阴性。本研究将Ki-67 水平的临界值定义为30%[7]。TNM 分期以及组织学分级由病理科医师分别参考第七版美国癌症联合会(American Joint Committee on Cancer,AJCC)乳腺癌分期指南以及Nottingham 组织学分级系统进行确定[13,14]。
3.自动乳腺超声检查:所有患者均在术前接受ABUS 检查。使用GE 公司生产的 Invenia ABUS 2.0 自动乳腺超声诊断系统进行检查,扫查端探头频率为6 ~15 MHz。患者取仰卧位,双臂上举,充分暴露双侧乳腺,由专职乳腺超声医师扫查患者双侧乳房,每侧乳房常规采集正中位、外侧位和内侧位3 个切面,对于较大的乳房进行额外的扫查。每一切面扫查结束后标记乳头位置,保存图像并传输至ABUS 工作站,对影像数据自动进行三维重建。由 2 名高年资乳腺超声医师参考第五版乳腺影像报告和数据系统(breast imaging reporting and data system,BI-RADS)与《自动乳腺容积超声技术专家共识(2022 版)》对ABUS 检查获取到的病灶图像进行评估[10,15],并记录病灶的多种特征,包括最大径(≤2.0 cm / 2.0 ~5.0 cm /≥5.0 cm)、形状(不规则/规则)、边缘(不光整/光整)、内部回声(低回声/混合回声)、后方回声(无改变/增强/衰减)、钙化(无/有)、高回声晕(无/有)、冠状面汇聚征(无/有)以及冠状面跳跃征(无/有)。意见不一致时由另一名具有20 年乳腺超声诊断经验的主任医师决定。
三、统计学分析
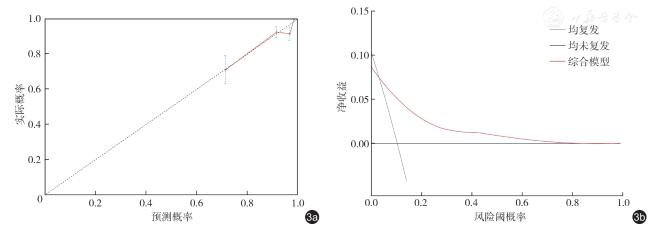
应用SPSS 26.0 和R 4.4.2 软件进行统计分析及模型构建。不符合正态分布的计量资料以M(Q1,Q3)表示,采用Mann-Whitney U 检验进行组间比较;计数资料以例数(%)表示,组间比较采用χ2 检验或Fisher 精确检验。采用多因素Cox回归分析Luminal B 型患者术后复发的独立风险因素,根据独立风险因素构建3 种预测模型,并计算各模型一致性指数(C-index),绘制ROC 曲线评估各模型预测性能,通过DeLong 检验比较3种模型的ROC 曲线下面积(area under the curve,AUC)。采用R 软件“rms”包绘制最佳模型的列线图,采用Bootstrap 法对最佳模型进行内部验证,绘制校准曲线对最佳模型性能进行评估,使用决策曲线评估最佳预测模型的临床获益。绘制不同复发风险因素特征患者的Kaplan-Meier 生存曲线,并进行Log-rank 检验。以P<0.05 为差异有统计学意义。
结 果
一、临床病理特征及ABUS 图像特征
本研究共纳入Luminal B 型乳腺癌患者293例(未复发组257 例,复发组36 例),中位年龄47 岁(年龄范围24 ~79 岁),62.5%(183/293)的患者在确诊时处于未绝经状态。治疗方面,73%(214/293)的患者接受了全乳切除术,43.7%(128/293)的患者于术前接受新辅助治疗,45.4%(133/293)的患者接受化疗,32.8%(96/293)的患者接受放疗。
此外,所有患者ER 表达均为阳性;86.7%(254/293)的患者PR 受体阳性,60.1%(176/293)Ki-67 百分比<30%; HER2 阴性100 例(34.1%,100/293),HER2 阳性193 例(65.9%,193/293)。
ABUS 测量的病灶最大径平均值为(2.92±1.75)cm;ABUS 图像观察到病灶形状不规则282 例(96.2%,282/293),边缘不光整283例(96.6%,283/293),内部回声为低回声283例(96.6%,283/293),伴有冠状面汇聚征205 例(70.0%,205/293)。未复发与复发患者N 分期、组织学分级、Ki-67 表达、肿瘤最大径、钙化以及冠状面跳跃征差异均有统计学意义(P<0.05,表1)。
表1 Luminal B 型乳腺癌患者术后未复发组与复发组临床病理及ABUS 图像特征比较[例(%)] |
| 特征 | 总计(n=293) | 未复发(n=257) | 复发(n=36) | 统计值 | P值 |
|---|---|---|---|---|---|
| 年龄[ 岁,M ( Q1, Q3 )] | 47.0(42.0,54.0) | 48.0(42.0,54.5) | 45.5(39.25,51.0) | Z=-1.831 | 0.067 |
| 绝经情况 | χ 2=0. 855 | 0.355 | |||
| 未绝经 | 183(62.5) | 158(61.5) | 25(69.4) | ||
| 已绝经 | 110(37.5) | 99(38.5) | 11(30.6) | ||
| 手术方式 | χ 2=0.568 | 0.494 | |||
| 保乳术后 | 79(27.0) | 71(27.6) | 8(22.2) | ||
| 全切术后 | 214(73.0) | 186(72.4) | 28(77.8) | ||
| 新辅助化疗 | χ 2=1.379 | 0.240 | |||
| 是 | 128(43.7) | 109(42.4) | 19(52.8) | ||
| 否 | 165(56.3) | 148(57.6) | 17(47.2) | ||
| 化疗 | χ 2=0.700 | 0.403 | |||
| 是 | 133(45.4) | 119(46.3) | 14(38.9) | ||
| 否 | 160(54.6) | 138(53.7) | 22(61.1) | ||
| 放疗 | χ 2=0.006 | 0.938 | |||
| 是 | 96(32.8) | 84(32.7) | 12(33.3) | ||
| 否 | 197(67.2) | 173(67.3) | 24(66.7) | ||
| T 分期 | χ 2=4.754 | 0.093 | |||
| 1 | 174(59.4) | 158(61.5) | 16(44.4) | ||
| 2 | 112(38.2) | 94(36.6) | 18(50) | ||
| 3 | 7(2.4) | 5(1.9) | 2(5.6) | ||
| N 分期 | χ 2=9.294 | 0.021 | |||
| 0 | 153(52.2) | 142(55.3) | 11(30.6) | ||
| 1 | 81(27.6) | 68(26.5) | 13(36.1) | ||
| 2 | 43(14.7) | 35(13.6) | 8(22.2) | ||
| 3 | 16(5.5) | 12(4.7) | 4(11.1) | ||
| PR 表达 | χ 2=0.012 | 0.913 | |||
| 阴性 | 39(13.3) | 34(13.2) | 5(13.9) | ||
| 阳性 | 254(86.7) | 223(86.8) | 31(86.1) | ||
| HER2 表达 | χ 2=0.233 | 0.629 | |||
| 阴性 | 100(34.1) | 89(34.6) | 11(30.6) | ||
| 阳性 | 193(65.9) | 168(65.4) | 25(69.4) | ||
| Ki-67 表达 | χ 2=5.794 | 0.016 | |||
| < 30% | 176(60.1) | 161(62.6) | 15(41.7) | ||
| ≥ 30% | 117(39.9) | 96(37.4) | 21(58.3) | ||
| 组织学分级 | χ 2=18.159 | < 0.001 | |||
| Ⅰ / Ⅱ级 | 256(87.4) | 233(90.7) | 23(63.9) | ||
| Ⅲ级 | 37(12.6) | 24(9.3) | 13(36.1) | ||
| 肿瘤最大径 | χ 2=7.683 | 0.021 | |||
| ≤ 2.0 cm | 100(34.1) | 94(36.6) | 6(16.7) | ||
| 2.0 ~ 5.0 cm | 163(55.6) | 140(54.5) | 23(63.9) | ||
| ≥ 5.0 cm | 30(10.2) | 23(8.9) | 7(19.4) | ||
| 形状 | χ 2=3.308 | 0.069 | |||
| 不规则 | 282(96.2) | 249(96.9) | 32(88.9) | ||
| 规则 | 11(3.8) | 8(3.1) | 3(8.3) | ||
| 边缘 | χ 2=0.05 | 0.823 | |||
| 不光整 | 283(96.6) | 248(96.5) | 35(97.2) | ||
| 光整 | 10(3.4) | 9(3.5) | 1(2.8) | ||
| 内部回声 | χ 2=0.05 | 0.823 | |||
| 低回声 | 283(96.6) | 248(96.5) | 35(97.2) | ||
| 混合回声 | 10(3.4) | 9(3.5) | 1(2.8) | ||
| 后方回声 | χ 2=1.862 | 0.394 | |||
| 无改变 | 199(67.9) | 178(69.3) | 21(58.3) | ||
| 增强 | 72(24.6) | 61(23.7) | 11(30.6) | ||
| 衰减 | 22(7.5) | 18(7.0) | 4(11.1) | ||
| 钙化 | χ 2=24.74 | < 0.001 | |||
| 无 | 190(64.8) | 180(70.0) | 10(27.8) | ||
| 有 | 103(35.2) | 77(30.0) | 26(72.2) | ||
| 高回声晕 | χ 2=0.121 | 0.728 | |||
| 无 | 163(55.6) | 142(55.3) | 21(58.3) | ||
| 有 | 130(44.4) | 115(44.7 | 15(41.7) | ||
| 冠状面汇聚征 | χ 2=0.99 | 0.753 | |||
| 无 | 88(30.0) | 78(30.4) | 10(27.8) | ||
| 有 | 205(70.0) | 179(69.6) | 26(72.2) | ||
| 冠状面跳跃征 | χ 2=14.905 | < 0.001 | |||
| 无 | 228(77.8) | 209(81.3) | 19(52.8) | ||
| 有 | 65(22.2) | 48(18.7) | 17(47.2) |
注:ABUS 为自动乳腺超声;PR 为孕激素受体;HER2 为人表皮生长因子受体2 |
二、Luminal B 型乳腺癌患者复发风险的多因素Cox 回归分析
将单因素分析中差异有统计学意义(P<0.05)的因子纳入多因素Cox 回归分析。经多因素分析,结果显示,N3 级(HR=3.762,95%CI:1.147 ~12.337,P=0.029)、组织学分级Ⅲ级(HR=3.558,95%CI:1.631 ~7.759,P=0.001)、钙化(HR=4.066,95%CI:1.888 ~8.757,P<0.001)与冠状面跳跃征(HR=2.178,95%CI:1.064 ~4.460,P=0.033)是Luminal B 型患者复发的独立风险因素(表2)。
表2 Luminal B 型乳腺癌患者术后复发的多因素Cox 回归分析 |
| 因素 | β值 | SE | Wald χ2值 | HR (95% CI ) | P值 |
|---|---|---|---|---|---|
| N 分期 | |||||
| 0 | Ref | ||||
| 1 | 0.597 | 0.417 | 2.047 | 1.817( 0.802 ~ 4.117) | 0.153 |
| 2 | 0.853 | 0.491 | 3.011 | 2.346( 0.895 ~ 6.147) | 0.083 |
| 3 | 1.325 | 0.606 | 4.779 | 3.762( 1.147 ~ 12.337) | 0.029 |
| Ki-67 表达 | |||||
| < 30% | Ref | ||||
| ≥ 30% | 0.490 | 0.368 | 1.772 | 1.632(0.793 ~ 3.358) | 0.183 |
| 组织学分级 | |||||
| Ⅰ / Ⅱ级 | Ref | ||||
| Ⅲ级 | 1.269 | 0.398 | 10.178 | 3.558( 1.631 ~ 7.759) | 0.001 |
| 肿瘤最大径 | |||||
| ≤ 2.0 cm | Ref | ||||
| 2.0 ~ 5.0 cm | 0.263 | 0.479 | 0.302 | 1.301( 0.509 ~ 3.327) | 0.583 |
| ≥ 5.0 cm | 0.299 | 0.616 | 0.236 | 1.349(0.403 ~ 4.509) | 0.627 |
| 钙化 | |||||
| 无 | Ref | ||||
| 有 | 1.403 | 0.391 | 12.835 | 4.066( 1.888 ~ 8.757) | <0.001 |
| 冠状面跳跃征 | |||||
| 无 | Ref | ||||
| 有 | 0.779 | 0.366 | 4.534 | 2.178(1.064 ~ 4.460) | 0.033 |
三、预测模型建立与验证
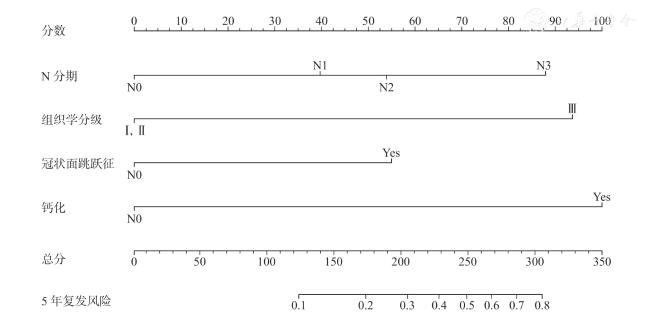
根据多因素Cox 回归分析结果进行模型构建。基于N 分期、组织学分级建立临床病理模型;基于钙化、冠状面跳跃征建立ABUS 图像模型;基于N 分期、组织学分级、钙化以及冠状面跳跃征建立综合模型。结果显示,各模型的C-index 分别为临床病理模型0.687(95%CI:0.593 ~0.781)、ABUS 模型0.734(95%CI:0.650 ~0.818)、综合模型0.791(95%CI:0.718 ~0.864,表3)。
表3 Luminal B 型乳腺癌术后复发的3 种预测模型效能分析 |
| 模型 | C-index(95%CI) | 准确性(95%CI) | 敏感度(95%CI) | 特异度(95%CI) |
|---|---|---|---|---|
| 临床病理模型 | 0.687(0.593 ~ 0.781) | 0.717(0.669 ~ 0.768) | 0.583(0.425 ~ 0.744) | 0.735(0.683 ~ 0.788) |
| ABUS 模型 | 0.734(0.650 ~ 0.818) | 0.611(0.560 ~ 0.669) | 0.833(0.708 ~ 0.943) | 0.580(0.521 ~ 0.640) |
| 综合模型 | 0.791(0.718 ~ 0.864) | 0.816(0.766 ~ 0.858) | 0.856(0.813 ~ 0.899) | 0.810(0.747 ~ 0.864) |
注:ABUS 为自动乳腺超声;C-index 为一致性指数 |
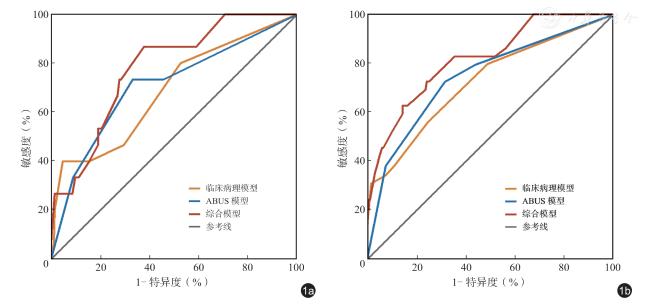
绘制各种模型随访3 年与随访5 年的ROC 曲线,结果显示,临床病理模型、ABUS 模型、综合模型的3 年AUC 分别为0.688、0.707、0.779,5 年AUC 分别为0.724、0.745、0.819( 图1)。DeLong 检验结果显示综合模型的5 年AUC 显著高于临床病理模型(Z=2.759,P=0.005)和ABUS图像模型(Z=2.13,P=0.033),差异有统计学意义。临床病理模型与ABUS 图像模型AUC 接近,差异无统计学意义(Z=0.867,P=0.386)。
四、生存分析
在中位随访时间为68(56,85)个月的随访中,257 例未发生复发,36 例患者发生复发,患者术后复发率为12.3%(36/293),复发中位时间为40.5(31.25,54.0)个月,3 年和5 年累积生存率分别为92.38%和88.47%。其中局部区域复发16例,远处转移20 例。
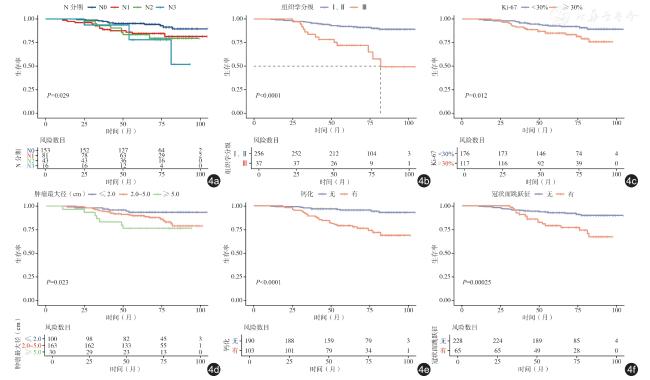
N 分期中N0、N1、N2、N3 分期患者3 年累积生存率分别为95%、88%、91%、94%,5年累积生存率分别94%、85%、79%、77%,不同N 分期之间的累积生存率差异有统计学意义(P=0.029)。组织学分级Ⅰ/Ⅱ级患者3 年和5 年累积生存率为94%和91%,Ⅲ级的患者为78%和71%,不同组织学分级之间的累积生存率差异有统计学意义(P<0.001)。Ki-67 低表达患者3 年和5 年累积生存率分别为95%和92%,而Ki-67 高表达患者分别为89%和83%,不同Ki-67 表达之间的累积生存率差异有统计学意义(P<0.012)。肿瘤最大径≤2.0 cm、2.0 ~5.0 cm、≥5.0 cm患者3 年累积生存率分别为96%、92%、83%,5年累积生存率分别为93%、88%、76%,不同肿瘤最大径之间的累积生存率差异有统计学意义(P=0.023)。无钙化患者3 年和5 年累积生存率分别为97%和96%,而有钙化的患者为84%和76%,有无钙化之间的累积生存率差异有统计学意义(P<0.001)。无冠状面跳跃征的患者3 年和5年累积生存率分别为94%和92%,有冠状面跳跃征的患者为86%和77%,有无冠状面跳跃征之间的累积生存率差异有统计学意义(P<0.001,表4、图4)。
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
图4 不同复发风险因素特征的Luminal B 型乳腺癌患者的术后生存曲线。图a 为不同N 分期患者的K-M 生存曲线;图b为不同组织学分级患者的K-M 生存曲线;图c 为Ki-67 高表达与Ki-67 低表达患者的K-M 生存曲线;图d 为不同肿瘤最大径患者的K-M 生存曲线;图e 为存在与不存在钙化患者的K-M 生存曲线;图f 为存在与不存在冠状面跳跃征患者的K-M生存曲线 |
表4 Luminal B 型乳腺癌患者生存分析 |
| 风险因素 | 例数 | 中位生存时间(月) | 累积生存率 | χ 2值 | P值 | |
|---|---|---|---|---|---|---|
| 3 年 | 5 年 | |||||
| N 分期 | 9.013 | 0.029 | ||||
| 0 | 153 | 71.00 | 95% | 94% | ||
| 1 | 81 | 64.00 | 88% | 85% | ||
| 2 | 43 | 67.00 | 91% | 79% | ||
| 3 | 16 | 56.50 | 94% | 77% | ||
| 组织学分级 | 23.713 | < 0.001 | ||||
| Ⅰ / Ⅱ级 | 256 | 70.00 | 94% | 91% | ||
| Ⅲ级 | 37 | 56.00 | 78% | 71% | ||
| Ki-67 | 6.355 | 0.012 | ||||
| 低表达 | 176 | 70.00 | 95% | 92% | ||
| 高表达 | 117 | 65.00 | 89% | 83% | ||
| 肿瘤最大径 | 7.579 | 0.023 | ||||
| ≤ 2.0 cm | 100 | 72.00 | 96% | 93% | ||
| 2.0 ~ 5.0 cm | 163 | 66.00 | 92% | 88% | ||
| ≥ 5.0 cm | 30 | 69.00 | 83% | 76% | ||
| 钙化 | 24.668 | < 0.001 | ||||
| 无 | 190 | 69.50 | 97% | 96% | ||
| 有 | 103 | 65.00 | 84% | 76% | ||
| 冠状面跳跃征 | 13.397 | < 0.001 | ||||
| 无 | 228 | 69.00 | 94% | 92% | ||
| 有 | 65 | 65.00 | 86% | 77% | ||
讨 论
大量的研究证明,淋巴结受累多、肿瘤体积大以及组织学分级高与乳腺癌患者的复发紧密相关[19,20]。本研究观察到随着N 分期的增高,复发风险随之增加,生存率下降;此外,经多因素分析N3 期(HR=3.762,P=0.029)是Luminal B 型乳腺癌患者复发的独立风险因素。Braunstein 等[21]研究显示,淋巴结阴性患者8 年复发风险为2.8%,而阳性患者为5.2%;此外,淋巴结受累状况与乳腺癌患者的复发风险呈正相关(4 ~9 个淋巴结受累HR=3.04,>9 个淋巴结受累HR=5.82,P<0.01)。本研究中,组织学分级Ⅲ级是Luminal B 型乳腺癌术后复发的独立风险因素(HR=3.558,P=0.001),5 年累积生存率较Ⅰ、Ⅱ级明显下降(91% vs 71%,P<0.001)。组织学分级是根据小管或腺体结构、核多形性和有丝分裂计数三种形态学特征进行评估,其中Ⅲ级代表肿瘤生长速度快,侵袭性高,具有较高的复发死亡风险[22]。Pan 等[20]的研究中发现复发风险随组织学分级的增加而增加(Ⅰ级10%、Ⅱ级13%、Ⅲ级17%)。当肿瘤体积较大时,病灶内产生大量的新生毛细血管,而新生毛细血管管壁结构不完全,通透性好,肿瘤细胞易通过血行播散进行转移;此外,较大的肿瘤手术清除难度大,易残留[23]。本研究发现,随着肿瘤体积增大,患者的累积生存率明显下降,即肿瘤最大径为2.0 ~5.0 cm及5.0 cm 以上的患者3 年及5 年累积生存率显著低于≤2.0 cm 的患者(P<0.05)。然而,在多因素分析中,肿瘤最大径并无统计学意义(P>0.05)。Ki-67 是反映细胞增殖可靠的生物标志物,并且高水平Ki-67 往往与不良预后相关[24],在本研究中,单因素分析表明,Ki-67 ≥30%与患者的不良预后相关(χ2=5.794,P=0.016)。具体而言,Ki-67 ≥30%患者的3 年和5 年的累积生存率显著低于Ki-67<30%(P<0.05)。但在多因素分析中,Ki-67 并无统计学意义(P>0.05)。
本研究观察到的ABUS 图像特征中,钙化(HR=4.066,P<0.001) 和冠状面跳跃征(HR=2.178,P=0.033)是复发的独立风险因素;通过生存分析发现,有钙化和有冠状面跳跃征的患者累积生存率均显著低于无钙化和无冠状面跳跃征患者(P<0.001)。Zheng 等[25]通过分析7000 多例中国女性的乳腺X 线摄影发现,有钙化的乳腺癌比无钙化的更具有侵袭性,并且预后更差;Li等[26]研究结果显示钙化灶是乳腺癌患者总生存期的独立风险因素(HR=1.95,P=0.026),与Qi等[27]的研究结果相似。冠状面成像是ABUS 独特的成像方式,其独特之处在于可通过单个切面展示整个乳房。冠状面汇聚征指病灶周边放射状分布的条状高回声向中心汇聚,可能是由肿瘤侵犯周围组织引起的收缩现象[28],有研究发现,Luminal 型乳腺癌更易出现冠状面汇聚征[29]。本研究中70%的Luminal B 型乳腺癌患者可观察到冠状面汇聚征,与既往研究结果一致。冠状面跳跃征表现为一条横向的无回声线,常见于组织硬度发生变化的位置,可能是由于换能器遇到坚硬的肿块,延缓探头设定的恒定移动速度,此时释放积聚的压力会导致探头在病变部位小幅跳跃或跳过[30,31]。本研究观察到的冠状面跳跃征仅限于病灶引起的情况,已排除由肋骨或致密乳腺产生的影响。虽然目前尚没有关于冠状面跳跃征与复发风险关系之间的报道,但这一现象可能与基质硬度有关。基质硬度是细胞外基质的机械特性,其在肿瘤中表现为从中心向周围递增,而基质硬度的增加可导致BCSC 的增加,进而激活相关信号通路(如YAP/TAZ),促进肿瘤复发与转移[32]。
Mao 等[33]基于乳腺X 线摄影建立的预测模型性能(AUC=0.78)与本研究相近,但乳腺X线摄影易受组织重叠的影响,对致密型乳腺的诊断敏感度较低;此外,患者接受度低,有研究表明,相较于乳腺X 线摄影(45.5%),92.4%的患者更愿意接受ABUS 检查[34]。Xu 等[35]基于动态对比增强磁共振成像(dynamic contrast enhancement magnetic resonance imaging,DCEMRI)中提取到的影像学特征、N 分期以及内分泌治疗情况,建立Luminal B 型乳腺癌术后复发的预测模型,其性能更优(5 年AUC=0.912),但MRI 的时间与经济成本高,限制了模型的广泛应用。Xiong 等[36]利用术前手持超声图像建立预测Luminal B 型乳腺癌患者复发风险的模型性能(C-index=0.796)与本研究的模型性能接近,但手持超声无法避免对操作者的依赖性,难以标准化,而ABUS 自动化、标准化的扫查方式克服了这一问题。本研究基于ABUS 图像特征联合临床病理特征,建立了临床病理模型、ABUS 图像模型以及综合模型,以预测Luminal B 型乳腺癌术后复发风险,3 种模型均表现出良好的预测性能(5年AUC:0.724 ~0.819)。其中综合模型性能最佳(C-index=0.791),相比于临床病理模型(0.717)和ABUS 模型(0.611),综合模型(0.861)提升了预测准确性;同时在区分未复发与复发患者时表现出较高的敏感度(0.856)与特异度(0.810),在识别复发与未复发患者方面具有一定的优势,漏诊率与假阳性率较低。此外,本研究建立的模型5 年AUC 均高于3 年AUC,这表明该模型的长期预测性能更好。值得注意的是,建立模型纳入的所有因素均为患者术前接受的必要的检查,无需进行额外的检查,显著降低了模型的应用成本,增强了临床可行性。虽然指南对随访方案及频率有明确规定,但缺乏针对不同复发风险患者的个性化管理,这可能导致高风险患者未能得到足够的关注与及时的干预;同时,低风险患者可能面临过度的随访,造成不必要的医疗资源浪费和患者负担。本研究建立的综合模型侧重于术后评估复发风险,为制定个体化随访方案提供科学依据;而ABUS 模型可在术前评估乳腺癌术后的复发风险,为医师选择合适的治疗方案提供参考。
本研究尚存在一些局限性:(1)本研究为单中心回顾性研究,缺乏外部验证,因此,在后续的研究中应扩大样本量并进行多中心、前瞻性研究,以提高模型性能并验证模型的泛化能力。(2)在确保样本量的前提下本研究将最短随访时间设定为3 年,虽然乳腺癌患者术后复发的第一个高峰期为2 ~3 年,但是术后5 年是第二个关键的复发节点,进一步延长随访时间有助于提升模型的长期预测性能。
综上所述,本研究基于ABUS 图像联合临床病理特征建立的预测模型具有较好的性能,该模型为预测Luminal B 型乳腺癌复发风险提供了一种高效、准确且经济的新方法,有助于临床医师评估复发风险以及制定个性化随访方案。