
新生儿卵巢囊肿发病率约为1%,一般在妊娠晚期通过产前超声检查发现,是产前超声检查中最常见的一种腹腔囊肿,其性质多为良性,部分可自行消退[1,2,3]。目前新生儿卵巢囊肿的发病机制尚不明确,多数学者认为与胎儿卵巢对胎盘或母体血液中发现的某些促性腺激素和雌激素的过度反应有关[4]。大部分新生儿卵巢囊肿在出生时无明显症状[5,6,7],需要引起注意的是,新生儿卵巢囊肿最常见的并发症是卵巢扭转,其发生率为38%~55%[8-9],且卵巢囊肿宫内陈旧性扭转发生率较高。解剖学研究表明,新生儿骨盆容积有限且卵巢支持韧带相对松弛,这一特殊解剖特征使卵巢囊肿容易进入腹腔,活动空间增大,继而增加了卵巢囊肿蒂扭转的风险[10]。鉴于卵巢囊肿蒂扭转可能导致不可逆的生殖功能损害,建立准确的早期诊断标准具有重要临床意义。因此,本研究对浙江大学医学院附属儿童医院60例婴幼儿卵巢囊肿进行分析,总结其超声表现特征,旨在为临床实践提供客观、可靠的诊断依据。
资料与方法
一、对象
回顾性选取2021年1月至2024年7月浙江大学医学院附属儿童医院收治的60例确诊为婴幼儿卵巢囊肿的病例。年龄范围:0~12个月。纳入标准:(1)年龄≤12月龄;(2)具有完整超声影像资料;(3)经手术病理检查或长期随访确诊。本研究经浙江大学医学院附属儿童医院伦理委员会审批通过:(批件号:2025-IRB-0112-P-01)。
二、方法
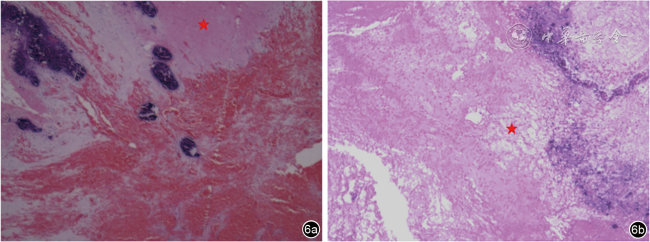
采用回顾性分析方法对60例研究对象的超声图像进行分析。超声特征及其病理表现的定义为:(1)钙化:将点状强回声称为钙化,可伴或不伴声影,一般在卵巢囊肿的囊壁可探及;钙化在病理切片中表现为特征性的深蓝色团块状沉积。(2)囊内分层:超声图像主要表现为液体分层征和回缩的团状中等回声,提示出血的发生;在病理切片中,出血表现为红细胞在血管腔外的聚集或含铁血黄素的沉着。(3)漩涡征样蒂结构:超声检查中漩涡征表现为特征性的螺旋状同心圆结构,部分病例可清晰显示扭转蒂部的连续性;其病理切片主要表现为胞质嗜酸性和细胞核的碎裂消失,伴或不伴局部出血钙化,提示组织存在缺血性坏死。计算超声特征的诊断敏感度、特异度、阳性预测值、阴性预测值、准确性,依据上述指标评估超声特征的诊断效能。
结果
一、病理及随访结果
60例确诊为卵巢囊肿的病例,根据病理结果及随访结果分为以下两类:(1)单纯性卵巢囊肿26例;(2)陈旧性卵巢囊肿蒂扭转34例,其中28例通过手术病理结果确诊,6例因随访发现自体截肢现象确诊。
二、婴幼儿陈旧性卵巢囊肿蒂扭转的超声特征及诊断效能

图1 婴幼儿陈旧性卵巢囊肿蒂扭转超声图像表现为钙化。图a为女性婴幼儿出生1个月,超声可见右侧腹囊性包块,内见液体分层征,囊壁可见散在环状钙化点(箭头所示),超声诊断右侧卵巢及囊肿陈旧性扭转坏死;图b为女性新生儿出生5 d,超声可见左侧腹囊实性包块,内见液体分层征,囊壁可见多发钙化斑(箭头所示),超声诊断左侧卵巢及囊肿陈旧性扭转坏死 |
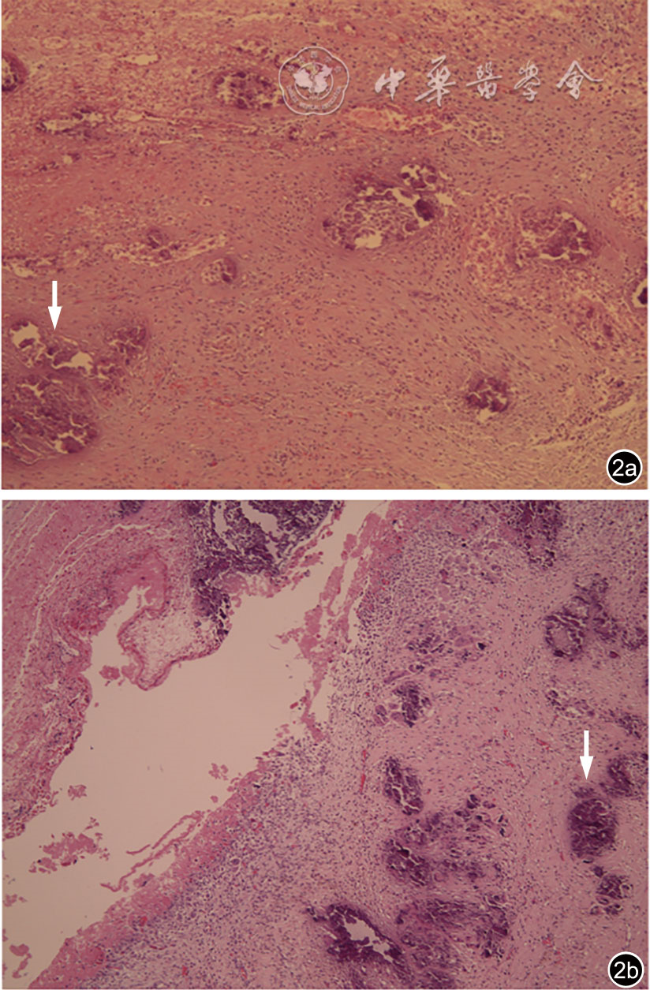
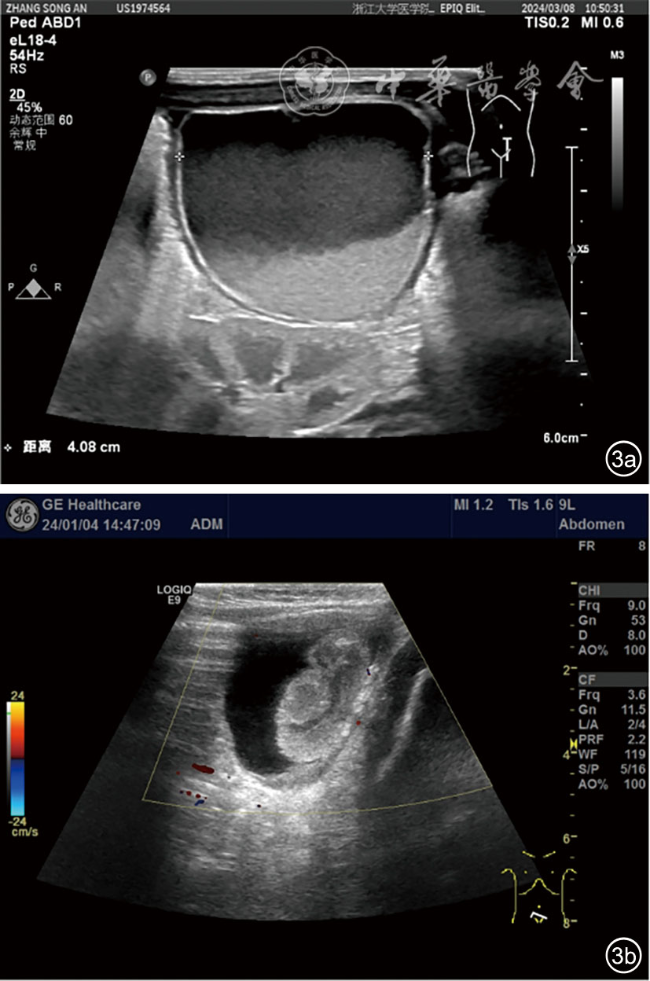
图3 婴幼儿陈旧性卵巢囊肿囊内分层超声图像。图a为女性婴幼儿,出生1个月,超声可见左下腹囊性包块,内见液体分层征,超声诊断左侧卵巢囊肿伴扭转;图b为女性婴幼儿,出生2个月,超声可见盆腔左侧囊实性包块,内见回缩样团块回声,囊壁可见斑片状钙化,超声诊断左侧卵巢来源囊肿及左侧卵巢陈旧性扭转坏死 |

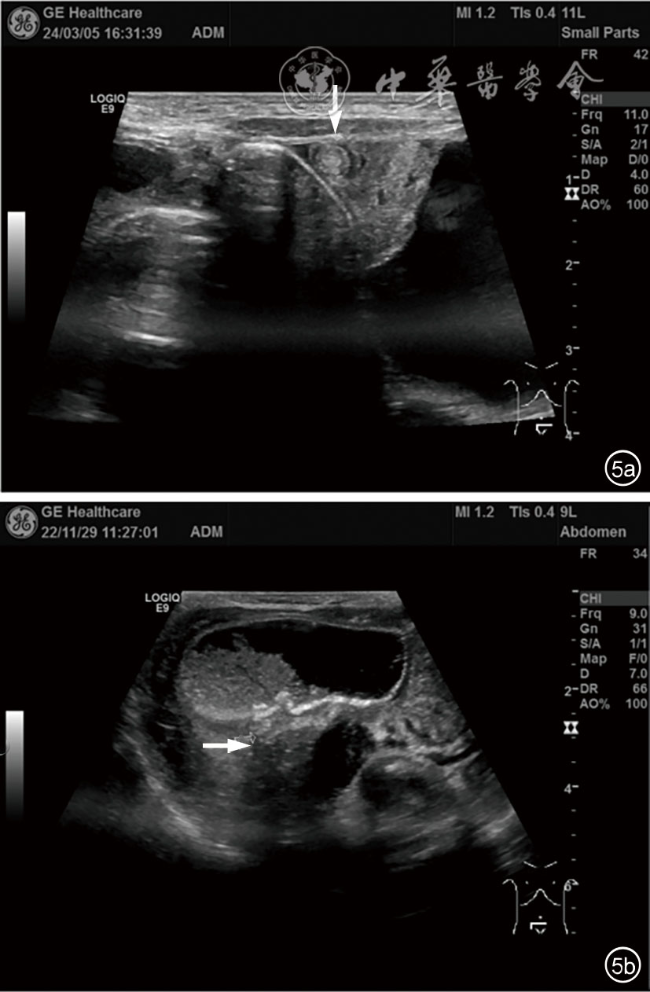
图5 婴幼儿陈旧性卵巢囊肿漩涡征样蒂结构超声图像。图a为女性新生儿,出生1 d,超声可见左中腹囊性包块,包块左下缘见螺旋样同心圆结构(箭头所示),扭转约360°,超声诊断左中腹囊性包块,左侧卵巢来源可能性大合并扭转考虑;图b为女性新生儿,出生8 d,超声可见右下腹囊性包块,内见液体分层征,包块后下缘低回声团,呈蒂样结构(箭头所示),超声诊断右侧卵巢来源囊肿及右侧卵巢陈旧性扭转坏死可能性大 |
4.钙化或囊内分层的诊断效能:本研究中存在钙化或囊内分层特征的病例共38例,其中31例确诊为陈旧性卵巢囊肿蒂扭转,其诊断敏感度为91.2%(31/34),特异度为73.1%(19/26),阳性预测值为81.6%(31/38),阴性预测值为86.4%(19/22)。
5.同时具备以上3种特征的诊断效能:本研究中同时存在钙化、囊内分层、漩涡征样蒂结构的病例共9例,全部确诊为陈旧性卵巢囊肿蒂扭转。3种特征同时具备的诊断敏感度为26.5%(9/34),特异度为100%(26/26),阳性预测值为100%(9/9),阴性预测值为51.0%(26/51)。
三、陈旧性卵巢囊肿蒂扭转的超声诊断准确性
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
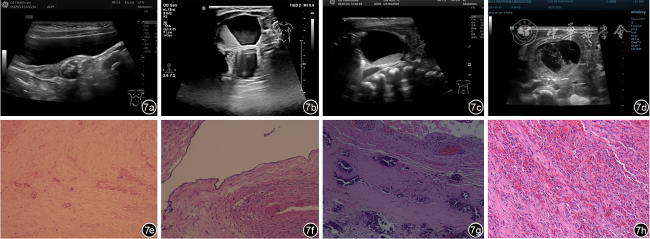
图7 陈旧性卵巢囊肿蒂扭转超声误诊病例超声及病理表现。图a为女性婴幼儿,出生12个月,超声可见盆腔内不均质团块回声,内见斑片状强回声伴声影,超声诊断左侧卵巢来源畸胎瘤;图b为女性婴幼儿,出生1个月,超声可见右侧附件区囊性包块,内见液体分层征,超声诊断右附件畸胎瘤;图c为女性新生儿,出生4 d,超声可见盆腔内囊实性包块,内见液体分层征,超声诊断盆腔囊实性包块,畸胎瘤待排;图d为女性新生儿,出生3 d,超声可见右侧腹囊性包块,内透声差,见分隔,超声诊断右侧腹囊性包块,肠重复畸形可能;图e(与图a为同一病例)病理提示左侧卵巢组织广泛坏死伴钙化改变,可见少许深蓝色团块状沉积和细胞核的碎裂消失(HE ×40);图f(与图b为同一病例)病理提示卵巢单纯性囊肿伴坏死钙化,可见散在细胞核的碎裂消失(HE ×100);图g(与图c为同一病例)病理提示卵巢囊肿蒂扭转伴坏死,可见深蓝色团块状沉积和红细胞在血管外聚集(HE ×200);图h(与图d为同一病例)病理提示卵巢囊肿蒂扭转伴出血坏死钙化,可见红细胞散在分布(HE ×200) |
讨论
本研究通过对60例婴幼儿卵巢囊肿病例的系统分析,发现34例为陈旧性卵巢囊肿蒂扭转,26例为单纯性卵巢囊肿,表明陈旧性卵巢囊肿蒂扭转在婴幼儿中的发病率并不低。为了更好地诊断婴幼儿陈旧性卵巢囊肿蒂扭转,本研究发现了陈旧性卵巢囊肿蒂扭转的3个关键诊断特征:(1)钙化(诊断特异度80.8%);(2)囊内分层(诊断特异度73.1%);(3)漩涡征样蒂结构(诊断特异度100%)。因此,如果发现婴幼儿卵巢囊肿的超声图像中出现这些特征,则要高度警惕其为陈旧性卵巢囊肿蒂扭转的可能性。值得注意的是,虽然漩涡征具有高度特异性(100%),但其敏感度相对较低(47.1%),这一现象可能归因于:(1)新生儿肠道气体干扰导致图像质量受限;(2)新生儿卵巢囊肿早期发生宫内扭转导致的蒂部纤维化改变难以在超声中辨别[11,12,13,14]。
此外,在诊断准确性评估中,有4例存在误诊,3例误诊为畸胎瘤,1例误诊为肠重复畸形。误诊为畸胎瘤的原因可能是因为卵巢畸胎瘤在儿童和青少年中的发病率较高[15-16],并且有些卵巢畸胎瘤的超声图像中也会出现液体分层征。但是实际上卵巢畸胎瘤在婴幼儿中是相对罕见的,多数研究统计的卵巢畸胎瘤病例平均发生年龄在11岁左右[17-18]。另外,卵巢畸胎瘤所呈现的液体分层征的超声特征通常在青春期后的患者中较为常见。最重要的是畸胎瘤特征性的超声表现其实是囊腔内结节样高回声伴声影(Rokitansky结节)[19]。所以当看到婴幼儿附件区的包块合并有钙化或囊内分层的超声表现时,应首先考虑为陈旧性卵巢囊肿蒂扭转而非畸胎瘤。
综上所述,在婴幼儿陈旧性卵巢囊肿蒂扭转的超声诊断中,钙化、囊内分层以及漩涡征样蒂结构的特征具有一定的应用价值。除漩涡征样蒂结构之外,还可以根据是否存在钙化、囊内分层来进行评估,而不一定局限于寻找漩涡征样蒂结构,这在一定程度解决了在实际超声检查中因漩涡征样蒂结构难以辨别而遗漏陈旧性卵巢囊肿蒂扭转的难题。