
2021 , Vol. 18 >Issue 10: 941 - 947
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2021.10.008
实时三维经食管超声心动图对二尖瓣脱垂的诊断价值
Copy editor: 汪荣
收稿日期: 2021-05-31
网络出版日期: 2021-10-27
基金资助
湖北省武汉市科技计划项目(2019020701011422)
武汉市卫生健康科研基金资助(WX21Q30)
版权
Diagnostic value of real-time three-dimensional transesophageal echocardiography for mitral valve prolaps
Received date: 2021-05-31
Online published: 2021-10-27
Copyright
比较实时三维经食管超声心动图(RT-3D-TEE)与二维经胸超声心动图(2D-TTE)、二维经食管超声心动图(2D-TEE)对二尖瓣脱垂的诊断价值。
回顾性分析2018年1月至2020年12月于武汉亚洲心脏病医院因二尖瓣脱垂行外科手术治疗,并在术前进行了2D-TTE、2D-TEE和RT-3D-TEE的患者共370例。以术中诊断为“金标准”,计算3种检查方法对二尖瓣脱垂瓣叶定位、腱索及赘生物形成的诊断效能,对3种检查方法的敏感度、特异度及准确性进行比较,并采用Kappa检验分别对3种方法诊断结果与术中诊断结果的一致性进行分析。
370例患者中,术前2D-TTE诊断出二尖瓣脱垂361例,检出率97.5%;术前2D-TEE诊断368例,检出率99.4%;而RT-3D-TEE检出率达100%。RT-3D-TEE对瓣叶脱垂的分区定位的敏感度、特异度和准确性均高于2D-TTE(P均<0.05),对腱索断裂诊断的敏感度和准确性亦高于2D-TTE,差异有统计学意义(P均<0.05),且RT-3D-TEE对脱垂分区定位的准确性高于2D-TEE(P均<0.05)。一致性分析结果显示,RT-3D-TEE各项指标与术中诊断均具有良好的一致性(Kappa值均>0.75,P均<0.05)。
RT-3D-TEE较2D-TTE、2D-TEE对二尖瓣脱垂区域的定位及相关病变的识别更准确,可为手术医师提供更为直观、精准的影像信息,帮助制定个性化治疗方案。
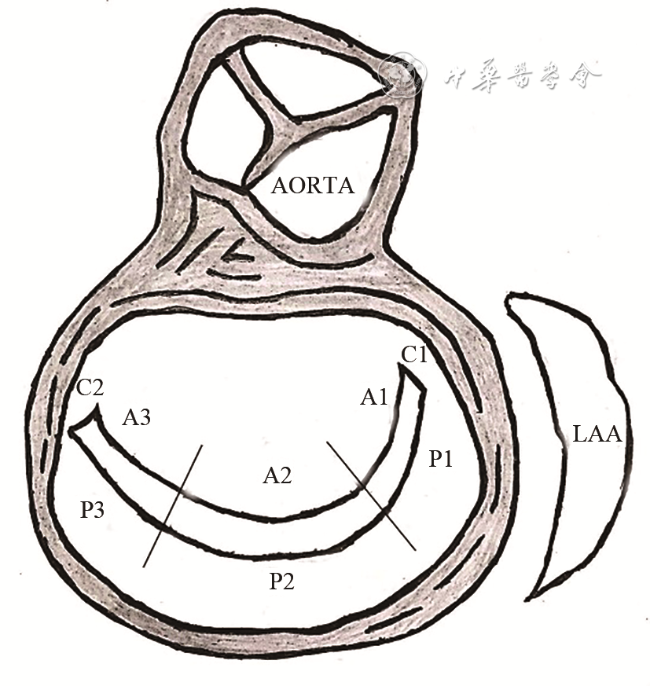
关键词: 二尖瓣脱垂; 成像,三维; 超声心动描记术,经食管
夏娟 , 马小静 , 谢姝瑞 , 何亚峰 , 程冠 , 吴梅 . 实时三维经食管超声心动图对二尖瓣脱垂的诊断价值[J]. 中华医学超声杂志(电子版), 2021 , 18(10) : 941 -947 . DOI: 10.3877/cma.j.issn.1672-6448.2021.10.008
To evaluate the value of real-time three-dimensional transesophageal echocardiography (RT-3D-TEE), two-dimensional transesophageal echocardiography (2D-TEE), and transthoracic echocardiography (2D-TTE) in the diagnosis of mitral valve prolapse (MVP).
A total of 370 patients with MVP diagnosed at Wuhan Asia Heart Hospital from January 2018 to December 2020 were analyzed retrospectively. The location of mitral valve prolapse, ruptured mitral chordae tendineae, and neoplasms were observed by 2D-TTE, 2D-TEE, and RT-3D-TEE, basing on the results of the surgery. The sensitivity, specificity, and accuracy of the three modalities were compared. The Kappa consistency test was used to compare the consistency with intraoperative diagnosis.
Compared with 2D-TTE, RT-3D-TEE had a higher sensitivity, specificity, and accuracy in determining the location of mitral valve prolapse (P<0.05), and RT-3D-TEE had a higher sensitivity and accuracy in diagnosis of ruptured mitral chordae tendineae (P<0.05). Compared with 2D-TEE, RT-3D-TEE had a higher accuracy in determining the location of mitral valve prolapse (P<0.05). RT-3D-TEE showed a good consistency with intraoperative diagnosis (Kappa values>0.75, P<0.05).
RT-3D-TEE is more accurate than 2D-TTE and 3D-TEE in the accurate localization of mitral valve prolapse. It can provide more intuitive and accurate information for surgeons to help guide treatment decisions.
表1 2D-TTE、2D-TEE及3D-TEE对二尖瓣脱垂分区及相关病变的诊断效能比较(%) |
| 病变区域 | 敏感度[例(%)] | χ2值 | P值 | 特异度[例(%)] | χ2值 | P值 | 准确性[例(%)] | χ2值 | P值 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2D-TTE | 2D-TEE | 3D-TEE | 2D-TTE | 2D-TEE | 3D-TEE | 2D-TTE | 2D-TEE | 3D-TEE | |||||||
| 二尖瓣脱垂 | |||||||||||||||
A1 | 92/114(80.7) | 105/114(92.1)a | 113/114(99.1)ab | 23.237 | 0.000 | 237/256(92.5) | 249/256(97.3)a | 256/256(100)ab | 22.054 | 0.000 | 329/370(88.9) | 354/370(95.7)a | 369/370(99.7)ab | 44.570 | 0.000 |
A2 | 103/141(72.7) | 132/141(93.6)a | 140/141(99.3)ab | 53.439 | 0.000 | 213/229(93.2) | 220/229(96.1) | 228/229(99.6)ab | 13.511 | 0.001 | 316/370(85.3) | 352/370(95.1)a | 368/370(99.5)ab | 61.622 | 0.000 |
A3 | 91/113(80.5) | 104/113(92.0)a | 112/113(99.1)ab | 23.258 | 0.000 | 241/257(94.0) | 247/257(96.1) | 256/257(99.6)ab | 13.126 | 0.001 | 332/370(89.7) | 351/370(94.9)a | 368/370(99.5)ab | 34.835 | 0.000 |
P1 | 70/91(76.7) | 84/91(92.2)a | 91/91(100)ab | 27.300 | 0.000 | 252/279(90.4) | 272/279(97.5)a | 279/279(100)ab | 36.114 | 0.000 | 322/370(87.0) | 356/370(96.2)a | 370/370(100)ab | 62.456 | 0.000 |
P2 | 127/152(83.4) | 142/152(93.4)a | 150/151(99.3)ab | 26.600 | 0.000 | 200/218(91.9) | 212/218(97.2) | 218/218(100)ab | 21.800 | 0.000 | 327/370(88.4) | 354/370(95.7)a | 369/370(99.7)ab | 47.889 | 0.000 |
P3 | 85/113(75.0) | 103/113(91.2)a | 112/113(99.1)ab | 32.857 | 0.000 | 234/257(91.2) | 251/257(97.6)a | 257/257(100)ab | 30.599 | 0.000 | 319/370(86.1) | 354/370(95.4)a | 369/370(99.7)ab | 61.879 | 0.000 |
C1 | 12/20(57.9) | 17/20(84.2) | 20/20(100)a | 10.909 | 0.004 | 320/350(91.4) | 336/350(96.0)a | 348/350(99.4)a | 26.918 | 0.000 | 332/370(89.7) | 353/370(95.4)a | 368/370(99.5)ab | 36.284 | 0.000 |
C2 | 21/34(60.6) | 28/34(81.8) | 33/34(97.10)a | 13.559 | 0.001 | 316/336(94.2) | 328/336(97.6)a | 335/336(99.7)a | 19.669 | 0.000 | 337/370(91.1) | 356/370(95.1)a | 368/370(99.5)ab | 31.300 | 0.000 |
| 腱索断裂 | 97/152(63.8) | 145/152(95.4)a | 149/152(98.0)a | 90.141 | 0.000 | 215/218(98.6) | 218/218(100) | 218/218(100) | 5.905 | 0.052 | 312/370(83.9) | 363/370(98.1)a | 367/370(99.2)a | 88.385 | 0.000 |
| 赘生物形成 | 11/13(84.6) | 12/13(92.3) | 13/13(100) | 2.167 | 0.338 | 354/357(99.1) | 356/357(99.7) | 357/357(100) | 3.513 | 0.173 | 365/370(98.6) | 368/370(99.4) | 370/370(100) | 5.463 | 0.065 |
注:2D-TTE为二维经胸超声心动图;2D-TEE为二维经食管超声心动图;RT-3D-TEE为实时三维经食管超声心动图;A1、A2、A3、P1、P2、P3、C1、C2为二尖瓣Carpentier分区;与2D-TTE相比,aP<0.017;与2D-TEE 相比,bP<0.017 |
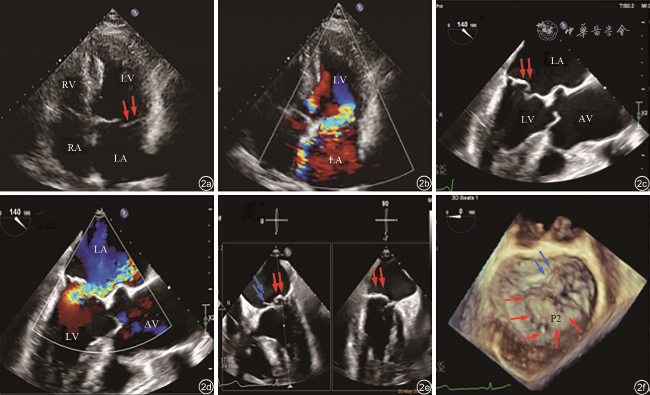
图2 二尖瓣P2区脱垂二维经胸超声心动图(2D-TTE)、二维经食管超声心动图(2D-TEE)和实时三维经食管超声心动图(RT-3D-TEE)检查图像。图a为2D-TTE显示二尖瓣后瓣P2区脱垂,未见明显腱索断裂;图b为2D-TTE显示二尖瓣口重度偏心性反流信号;图c为2D-TEE显示后瓣P2区脱垂,未见明显腱索断裂;图d为2D-TEE显示二尖瓣口重度偏心性反流信号;图e(对应动态图1)为RT-3D-TEE在两个正交平面同时观察到P2区的脱垂和腱索断裂;图f(对应动态图2)为左心房面外科视野观,三维立体结构实时显示脱垂区域和腱索断裂 |
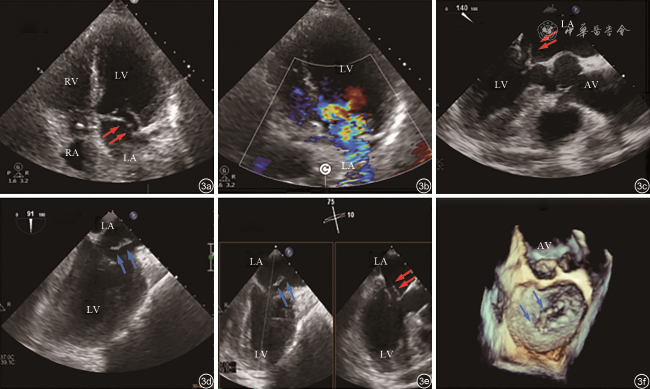
图3 二尖瓣A2区脱垂二维经胸超声心动图(2D-TTE)、二维经食管超声心动图(2D-TEE)和实时三维经食管超声心动图(RT-3D-TEE)超声检查图像。图a为2D-TTE显示前瓣A2区脱垂和腱索断裂,乳头肌断裂不明显;图b为2D-TTE显示二尖瓣口重度偏心性反流信号;图c为2D-TEE显示前瓣A2区脱垂;图d为2D-TEE显示断裂的乳头肌;图e(对应动态图3)为RT-3D-TEE在两个正交平面同时观察到A2区的脱垂和乳头肌断裂;图f(对应动态图4)为左心房面外科视野观,三维立体结构实时显示脱垂区域和乳头肌断裂 |
表2 2D-TTE、2D-TEE及3D-TEE诊断二尖瓣脱垂及相关病变与术中诊断的一致性分析 |
| 病变 | Kappa值 | ||
|---|---|---|---|
| 2D-TTE与术中诊断 | 2D-TEE与术中诊断 | RT-3D-TEE与术中诊断 | |
| 二尖瓣脱垂 | |||
A1 | 0.738 | 0.898 | 0.994 |
A2 | 0.681 | 0.897 | 0.989 |
A3 | 0.754 | 0.879 | 0.987 |
P1 | 0.658 | 0.898 | 1.000 |
P2 | 0.758 | 0.910 | 0.989 |
P3 | 0.671 | 0.897 | 0.994 |
C1 | 0.339 | 0.643 | 0.950 |
C2 | 0.511 | 0.719 | 0.968 |
| 腱索断裂 | 0.658 | 0.961 | 0.983 |
| 赘生物形成 | 0.808 | 0.920 | 1.000 |
注:2D-TTE为二维经胸超声心动图;2D-TEE为二维经食管超声心动图;RT-3D-TEE为实时三维经食管超声心动图;A1、A2、A3、P1、P2、P3、C1、C2为二尖瓣Carpentier分区 |
| 1 |
DeBonis M, Al-Attar N, Antunes M, et al. Surgical and interventional management of mitral valve regurgitation: a position statement from the European society of cardiology working groups on cardiovascular surgery and valvular heart disease [J]. Eur Heart J, 2016, 37(2): 133-139.
|
| 2 |
Feldman T, Kar S, Rinaldi M, et al. Percutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge repair Study) cohort [J]. J Am Coll Cardiol, 2009, 54(8): 686-694.
|
| 3 |
Sugeng L, Shernan SK, Salgo IS, et al. Live 3-dimensional transesophageal echocardiography initial experience using the fully sampled matrix array probe [J]. J Am CollCardiol, 2008, 52(6): 446-449.
|
| 4 |
Poelaert JI, Bouchez S. Perioperative echocardiographic assessment of mitral valve regurgitation:a comprehensive review [J]. Eur J Cardiothorac Surg, 2016, 50(5): 801-812.
|
| 5 |
王新房. 超声心动图学 [M]. 4版. 北京: 人民卫生出版社, 2009: 320-331.
|
| 6 |
Vavuranakis M, Kalogeras K, Lozos V, et al. Transapical closure of multiple mitral paravalvular leaks with dual device deployment through a single sheath: a Heart Team job [J]. Hellenic J Cardiol, 2018, 59(6): 367-369.
|
| 7 |
缪云翔, 赵彩明, 周炳元, 等. 经胸超声心动图在二尖瓣脱垂定位中的应用 [J]. 中国医学影像学杂志, 2020, 28(8): 591-594.
|
| 8 |
Faletra FF, Berrebi A, Pedrazzini G, et al. 3D transesophageal echocardiography: a new imaging tool for assessment of mitral regurgitation and for guiding percutaneous edge-to-edge mitral valve repair [J]. Prog Cardiovasc Dis, 2017, 60(3): 305-321.
|
| 9 |
张玲芳, 郑哲岚, 牟芸, 等. 实时三维经食管超声心动图对二尖瓣成形术的指导意义 [J/CD]. 中华医学超声杂志(电子版), 2018, 15(3): 198-203.
|
| 10 |
李昱茜, 徐学增, 白炜, 等. 实时三维经食管超声指导下全胸腔镜技术二尖瓣成形术的中短期随访效果评价 [J/CD]. 中华医学超声杂志(电子版), 2020, 17(5): 427-433.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}