
2022 , Vol. 19 >Issue 11: 1187 - 1192
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2022.11.006
超声对晚发型胎儿生长受限不良围产期结局的预测价值
Copy editor: 吴春凤
收稿日期: 2021-09-15
网络出版日期: 2023-01-19
基金资助
河南省医学适宜技术推广项目(SYJS2022066)
版权
Value of ultrasound in predicting pregnancy outcome of late-onset fetal growth restriction
Received date: 2021-09-15
Online published: 2023-01-19
Copyright
探讨超声对晚发型胎儿生长受限(FGR)不良围产期结局的预测因素,并分析其诊断效能。
回顾性分析2015年12月至2021年5月郑州大学第三附属医院收治的149例产前诊断为晚发型FGR患者的超声声像图及临床资料,按照是否出现不良围产期结局分为不良围产期结局组(72例)和对照组(77例)。记录一般临床资料及分娩前1周内经超声测量的大脑中动脉搏动指数(MCA-PI)、脐动脉搏动指数(UA-PI)、脑胎盘比(CPR)、羊水-脐脑比(AUCR)及估计胎儿体质量(EFW)。采用两独立样本t检验、Mann-Whitney U检验、χ2检验比较组间上述指标的差异,采用单因素和多因素Logistic逐步回归分析确定晚发型FGR不良围产期结局的预测因素,构建受试者操作特征(ROC)曲线分析各超声参数对不良围产期结局的预测效能。
与对照组相比,不良围产期结局组AUCR、EFW百分位数、CPR、MCA-PI、最大羊水暗区垂直深度均明显降低[30.63±10.33 vs 39.70±11.15;3.2(2.1,6.4)vs 5.7(3.5,8.9);1.18±0.28 vs 1.37±0.21;1.22±0.26 vs 1.34±0.23;27.50(22.00,31.00)mm vs 29.00(23.50,34.50)mm],UA-PI明显增高(1.05±0.20 vs 0.98±0.16),差异具有统计学意义(t=5.138,P<0.001;Z=-4.618,P<0.001;t=4.464,P<0.001;t=3.129,P=0.002;Z=-2.292,P=0.022;t=-2.504,P=0.013)。多因素Logistic逐步回归分析显示AUCR、EFW百分位数、CPR为晚发型FGR不良围产期结局的独立预测因素(OR=0.951、0.753、0.154,P=0.024、<0.001、=0.044)。经过ROC曲线分析,AUCR、EFW百分位数、CPR预测晚发型FGR不良围产期结局的界值、敏感度、特异度分别为39.64、53.2%、81.9%;4.85、66.2%、66.7%;1.19、81.8%、51.4%。AUCR、EFW百分位数、CPR 3个变量联合的多参数模型对不良围产期结局的诊断效能提升,弥补了单项参数预测晚发型FGR不良围产期结局敏感度与特异度失衡的问题,ROC曲线下面积为0.795,敏感度、特异度分别为76.6%、70.8%。
超声检查在预测晚发型FGR不良围产期结局中具有重要价值,AUCR、EFW百分位数及CPR是晚发型FGR不良围产期结局的独立预测因素,可为产前咨询和临床处理提供依据。
关键词: 超声; 胎儿生长受限; 妊娠结局; 脑胎盘比; 最大羊水暗区垂直深度
侯留杰 , 栗河舟 , 张红彬 , 张恒静 , 王昭宇 , 魏亚楠 . 超声对晚发型胎儿生长受限不良围产期结局的预测价值[J]. 中华医学超声杂志(电子版), 2022 , 19(11) : 1187 -1192 . DOI: 10.3877/cma.j.issn.1672-6448.2022.11.006
To explore the predictive factors of ultrasound for the adverse perinatal outcome of late-onset fetal growth restriction (FGR) and analyze their diagnostic efficacy.
A retrospective analysis was performed on the ultrasound images and clinical data of 149 patients with late-onset FGR who were admitted to the Third Affiliated Hospital of Zhengzhou University from December 2015 to May 2021. According to whether there were adverse perinatal outcomes, the patients were divided into an adverse perinatal outcome group (72 cases) and a control group (77 cases). General clinical data and middle cerebral artery pulsatility index (MCA-PI), umbilical artery pulsatility index (UA-PI), brain-placental rate (CPR), amniotic fluid-umbilical brain rate (AUCR), and estimated fetal weight (EFW) within one week before delivery were recorded. Two independent samples t-test, Mann-Whitney U test, and χ2 test were used to compare the differences in the above indicators between the groups, and the ROC curve was plotted to analyze the predictive performance of each ultrasound parameter on the adverse perinatal outcome, and single factor and multivariate logistic regression analyses were used to identify the meaningful predictors.
Compared with the control group, the AUCR, EFW percentile, CPR, MCA-PI, and MVP of the adverse perinatal outcome group were significantly lower [30.63±10.33 vs 39.70±11.15, t=5.138, P<0.001; 3.2 (2.1, 6.4) vs 5.7 (3.5, 8.9), Z=-4.618, P<0.001; 1.18±0.28 vs 1.37±0.21, t=4.464, P<0.001; 1.22±0.26 vs 1.34±0.23, t=3.129, P=0.002; 27.50 (22.00, 31.00) mm vs 29.00 (23.50, 34.50) mm, Z=-2.292, P=0.022], and UA-PI was significantly higher (1.05±0.20 vs 0.98±0.16, t=-2.504, P=0.013). Multivariate logistic regression analysis showed that AUCR, EFW percentile, and CPR were independent predictors of poor perinatal outcome of late-onset FGR (odds ratio=0.951, 0.753, and 0.154; P=0.024,<0.001, and =0.044, respectively). ROC curve analysis showed that the cut-off value, sensitivity, and specificity of AUCR, EFW percentile, and CPR for predicting adverse perinatal outcome of late-onset FGR were 39.64, 53.2%, and 81.9%, 4.85, 66.2%, and 66.7%, and 1.19, 81.8%, and 51.4%, respectively. Multi-parameter model including AUCR, EFW percentiles, and CPR had improved diagnostic performance for poor perinatal outcomes, and made up for the imbalance between sensitivity and specificity of single parameter in predicting adverse perinatal outcomes of late-onset FGR. The area under the ROC curve of the model was 0.795, and the sensitivity and specificity were 76.6% and 70.8%, respectively.
Ultrasonography is of great value in predicting the adverse perinatal outcome of late-onset FGR. AUCR, EFW percentile, and CPR are independent predictors of adverse perinatal outcome of late-onset FGR, providing a basis for prenatal consultation and clinical management.
表1 2组晚发型胎儿生长受限孕妇及新生儿一般临床资料比较 |
| 组别 | 例数 | 超声诊断孕周[周,M(QR)] | 终止妊娠孕周[周,M(QR)] | 新生儿性别(男/女,例) | 新生儿出生体质量[g,M(QR)] | Apgar-1[分,M(QR)] | Apgar-5[分,M(QR)] |
|---|---|---|---|---|---|---|---|
| 不良围产期结局组 | 72 | 33.57(33.00,34.54) | 34.64(33.71,35.86) | 43/29 | 1600(1400,1787) | 9(9,10) | 10(9,10) |
| 对照组 | 77 | 34.71(33.79,36.00) | 36.86(35.14,38.00) | 44/33 | 2100(1755,2360) | 10(9,10) | 10(10,10) |
| 统计值 | Z=-4.247 | Z=-5.571 | χ2=0.102 | Z=-6.750 | Z=-4.361 | Z=-3.806 | |
| P值 | <0.001 | <0.001 | 0.750 | <0.001 | <0.001 | <0.001 | |
| 组别 | 例数 | 年龄(岁, ±s) | 孕期增加体质量[kg,M(QR)] | 初产妇[例(%)] | 子痫前期[例(%)] | 剖宫产[例(%)] | 超声诊断孕周[周,M(QR)] |
| 不良围产期结局组 | 72 | 30.5±4.1 | 12.00(10.00,15.00) | 35(48.6) | 45(62.5) | 62(86.1) | 33.57(33.00,34.54) |
| 对照组 | 77 | 29.5±4.3 | 13.00(10.00,15.00) | 41(53.2) | 32(41.6) | 59(76.6) | 34.71(33.79,36.00) |
| 统计值 | t=-1.450 | Z=-1.336 | χ2=0.320 | χ2=6.534 | χ2=2.195 | Z=-4.247 | |
| P值 | 0.149 | 0.182 | 0.572 | 0.011 | 0.138 | <0.001 |
注:Apgar-1为新生儿第1分钟Apgar评分;Apgar-5为新生儿第5分钟Apgar评分 |
表2 2组晚发型生长受限胎儿各项超声参数比较 |
| 组别 | 例数 | EFW<第3百分位数[例(%)] | EFW百分位数[M(QR)] | MCA-PI( ±s) | UA-PI( ±s) | MVP[mm,M(QR)] | CPR( ±s) | AUCR( ±s) |
|---|---|---|---|---|---|---|---|---|
| 不良围产期结局组 | 72 | 36(50.0) | 3.2(2.1,6.4) | 1.22±0.26 | 1.05±0.20 | 27.50(22.00,31.00) | 1.18±0.28 | 30.63±10.33 |
| 对照组 | 77 | 18(23.4) | 5.7(3.5,8.9) | 1.34±0.23 | 0.98±0.16 | 29.00(23.50,34.50) | 1.37±0.21 | 39.70±11.15 |
| 统计值 | χ2=11.413 | Z=-4.618 | t=3.129 | t=-2.504 | Z=-2.292 | t=4.464 | t=5.138 | |
| P值 | 0.001 | <0.001 | 0.002 | 0.013 | 0.022 | <0.001 | <0.001 |
注:EFW为胎儿估计体质量;MVP为最大羊水暗区垂直深度;MCA-PI为大脑中动脉搏动指数;UA-PI为脐动脉搏动指数;CPR为脑胎盘率;AUCR为羊水-脐脑率 |
表3 晚发型生长受限胎儿各项超声参数单因素Logistic回归分析结果 |
| 自变量 | 回归系数 | 标准误 | Wald | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| AUCR | -0.079 | 0.018 | 19.666 | <0.001 | 0.924 | 0.893~0.957 |
| EFW百分位数 | -0.294 | 0.066 | 19.660 | <0.001 | 0.746 | 0.655~0.849 |
| CPR | -3.097 | 0.749 | 17.104 | <0.001 | 0.045 | 0.010~0.196 |
| UA-PI | 2.336 | 0.964 | 5.874 | 0.015 | 10.335 | 1.563~68.328 |
| MCA-PI | -2.124 | 0.716 | 8.792 | 0.003 | 0.120 | 0.029~0.487 |
| MVP | -0.068 | 0.026 | 7.043 | 0.008 | 0.934 | 0.888~0.982 |
注:EFW为胎儿估计体质量;MVP为最大羊水暗区垂直深度;MCA-PI为大脑中动脉搏动指数;UA-PI为脐动脉搏动指数;CPR为脑胎盘率;AUCR为羊水-脐脑率 |
表4 晚发型生长受限胎儿各项超声参数多因素Logistic逐步回归分析结果 |
| 自变量 | 回归系数 | 标准误 | Wald | P值 | OR值 | 95%CI |
|---|---|---|---|---|---|---|
| AUCR | -0.050 | 0.022 | 5.090 | 0.024 | 0.951 | 0.910~0.993 |
| EFW百分位数 | -0.283 | 0.073 | 15.181 | <0.001 | 0.753 | 0.653~0.869 |
| CPR | -1.874 | 0.930 | 4.064 | 0.044 | 0.154 | 0.025~0.949 |
注:EFW为胎儿估计体质量;CPR为脑胎盘率;AUCR为羊水-脐脑率 |
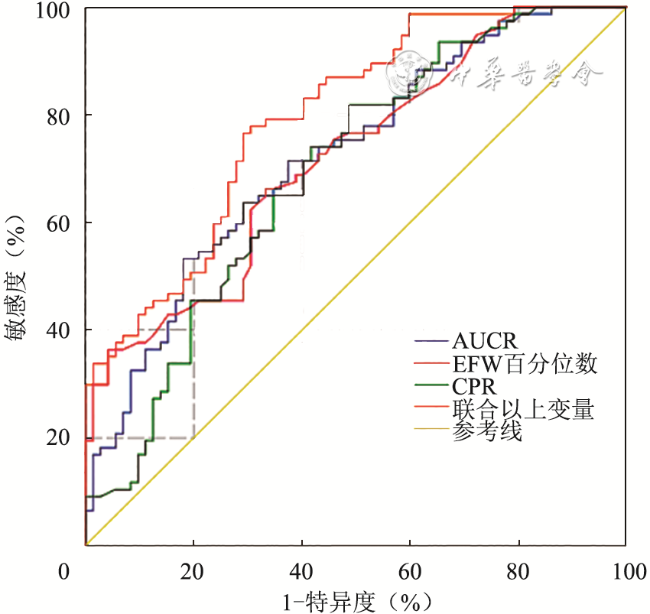
表5 胎儿各项超声参数对晚发型FGR不良围产期结局的预测价值 |
| 参数 | 曲线下面积 | 95%CI | 界值 | 敏感度(%) | 特异度(%) |
|---|---|---|---|---|---|
| AUCR | 0.722 | 0.641~0.802 | 39.64 | 53.2 | 81.9 |
| EFW百分位数 | 0.719 | 0.639~0.800 | 4.85 | 66.2 | 66.7 |
| CPR | 0.692 | 0.607~0.777 | 1.19 | 81.8 | 51.4 |
| 联合三个变量 | 0.795 | 0.725~0.865 | 0.51 | 76.6 | 70.8 |
注:AUCR为羊水-脐脑率,EFW为胎儿估计体质量,CPR为脑胎盘率 |
| 1 |
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
|
| 8 |
|
| 9 |
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
王晓静, 马颖, 张雅丽. 妊娠晚期特发性羊水偏少孕妇羊水成分变化及对妊娠结局的影响 [J]. 中国计划生育学杂志, 2018, 26(6): 494-499.
|
| 15 |
|
| 16 |
|
| 17 |
|
/
| 〈 |
|
〉 |


{kind=link}
{kind=link}