
2023 , Vol. 20 >Issue 05: 517 - 523
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.05.009
超声对易误诊的等回声、高回声甲状腺结节良恶性的鉴别
Copy editor: 吴春凤
收稿日期: 2022-06-09
网络出版日期: 2023-10-06
版权
Differential diagnosis of easily misdiagnosed benign and malignant isoechoic and hyperechoic thyroid nodules by ultrasound
Received date: 2022-06-09
Online published: 2023-10-06
Copyright
评价超声鉴别等回声、高回声甲状腺结节良恶性的价值。
回顾性分析2019年8月至2020年12月在苏州大学附属第三医院经手术病理证实的128个等回声、高回声甲状腺结节的超声声像图资料。以病理结果为金标准,将甲状腺结节分为良性组(n=94)和恶性组(n=34)。评估结节的超声特征,包括回声、边缘、生长方式、钙化、声晕、回声质地、后方回声、结中结表现、囊性变和血流。采用独立样本t检验、χ2检验或Fisher精确检验比较良恶性组间超声特征的差异。绘制受试者操作特征(ROC)曲线,计算曲线下面积(AUC)分析各超声特征参数的诊断效能。
恶性组中结节边缘不光整(38.2% vs 5.3%,P<0.001)、垂直位生长(17.6% vs 2.1%,P=0.004)、含有钙化(73.5% vs 17.0%,P<0.001)、回声质地不均匀(94.1% vs 55.3%,χ2=16.53,P<0.001)、少许血流(79.4% vs 57.4%,P=0.017)均较良性组多见,且差异均具有统计学意义。有、无声晕在良恶性组间差异无统计学意义(P>0.05),但在有声晕的结节中,声晕厚度不一致(84.2% vs 8.2%,χ2=37.58,P<0.001)提示与恶性相关。结节回声质地不均匀诊断敏感度最高,为94.12%,垂直位生长诊断特异度最高,为97.87%,声晕厚度不一致的AUC和诊断准确性最高,分别为0.880和89.71%。
等回声、高回声甲状腺结节边缘不光整、垂直位生长、存在粗大钙化或微钙化、声晕厚度不一致、回声质地不均匀以及少许血供有助于诊断恶性结节。
付泽辉 , 王思齐 , 卢叶君 , 张剑 , 贺烨 , 陈卉 . 超声对易误诊的等回声、高回声甲状腺结节良恶性的鉴别[J]. 中华医学超声杂志(电子版), 2023 , 20(05) : 517 -523 . DOI: 10.3877/cma.j.issn.1672-6448.2023.05.009
To evaluate the diagnostic value of ultrasound in isoechoic and hyperechoic thyroid nodules.
A retrospectively analysis was performed on the ultrasonographic data of 128 cases of isoechoic and hyperechoic thyroid nodules confirmed by surgery and pathology at the Third Affiliated Hospital of Soochow University from August 2019 to December 2020. Based on the pathological results as the gold standard, there were 94 cases of benign nodules and 34 cases of malignant nodules. The ultrasonic features of nodules, including echo, margin, growth mode, calcification, halo, echo texture, posterior echo, nodule-in-nodule architecture, cystic change, and blood flow, were evaluated. Independent sample t-test, χ2 test, or Fisher's exact test was used for statistical comparison of ultrasonic features between groups. The diagnostic efficacy of each parameter was analyzed using the receiver operating characteristic (ROC) curve and the area under curve (AUC).
In the benign and malignant groups, irregular margin of the nodule (38.2% vs 5.3%, P<0.001), vertical growth (17.6% vs 2.1%, P=0.004), calcification (73.5% vs 17.0%, P<0.001), uneven echo texture (94.1% vs 55.3%, χ2=16.53, P<0.001), and a little blood flow (79.4% vs 57.4%, P=0.017) all suggested the risk of malignancy. There was no difference in the presence or absence of halo between the two groups (P>0.05). In nodules with halo, inconsistent halo thickness (84.2% vs 8.2%, χ2=37.58, P<0.001) suggested the risk of malignancy. The diagnostic sensitivity of uneven echo texture of nodules (94.12%) was the highest, and the diagnostic specificity of vertical growth (97.87%) was the highest. The AUC and diagnostic accuracy of inconsistent sound halo thickness were the highest (0.880 and 89.71%, respectively).
Isoechoic and hyperechoic nodules with irregular edges, vertical growth, coarse calcification or microcalcification, inconsistent thickness of acoustic halo, uneven echo texture, and a little blood supply are helpful to the diagnosis of malignant nodules.
Key words: Ultrasound; Isoechoic; Hyperechoic; Thyroid nodules; Diagnostic value
表1 良、恶性甲状腺结节组患者基本临床资料比较 |
| 组别 | 例数 | 年龄(岁, ±s) | 最大径(cm, ±s) | 男[例(%)] | 女[例(%)] |
|---|---|---|---|---|---|
| 良性组 | 94 | 51.1±12.7 | 3.3±1.6 | 14(15.6) | 76(84.4) |
| 恶性组 | 34 | 45.4±14.6 | 2.2±1.7 | 10(30.3) | 23(69.7) |
| 统计值 | t=2.121 | t=3.172 | χ2=3.32 | ||
| P值 | 0.036 | 0.002 | 0.069 | ||
表2 良、恶性甲状腺结节超声特征比较[个(%)] |
| 特征 | 良性组(n=94) | 恶性组(n=34) | 统计值 | P值 |
|---|---|---|---|---|
| 回声 | χ2=0.03 | 0.857 | ||
| 等回声 | 76(80.9) | 27(79.4) | ||
| 高回声 | 18(19.1) | 7(20.6) | ||
| 边缘 | - | <0.001* | ||
| 光整 | 89(94.7) | 21(61.8) | ||
| 不光整 | 5(5.3) | 13(38.2) | ||
| 生长方式 | - | 0.004* | ||
| 水平位 | 92(97.9) | 28(82.4) | ||
| 垂直位 | 2(2.1) | 6(17.6) | ||
| 钙化 | - | <0.001* | ||
| 无 | 78(83.0) | 9(26.5) | ||
| 粗大钙化 | 9(9.6) | 6(17.6) | ||
| 微钙化 | 7(7.4) | 19(55.9) | ||
| 声晕 | χ2=0.14 | 0.707 | ||
| 无 | 45(47.9) | 15(44.1) | ||
| 有 | 49(52.1) | 19(55.9) | ||
| 声晕厚度# | χ2=37.58 | <0.001 | ||
| 一致 | 45(91.8) | 3(15.8) | ||
| 不一致 | 4(8.2) | 16(84.2) | ||
| 回声质地 | χ2=16.53 | <0.001 | ||
| 均匀 | 42(44.7) | 2(5.9) | ||
| 不均匀 | 52(55.3) | 32(94.1) | ||
| 后方回声 | - | - | ||
| 无改变 | 94(100) | 34(100) | ||
| 增强或衰减 | 0(0) | 0(0) | ||
| 结中结 | - | 0.475* | ||
| 无 | 86(91.5) | 32(94.1) | ||
| 有 | 8(8.5) | 2(5.9) | ||
| 囊性变 | χ2=2.26 | 0.131 | ||
| 无 | 75(79.8) | 31(91.2) | ||
| 有 | 19(20.2) | 3(8.8) | ||
| CDFI | - | 0.017* | ||
| 无 | 6(6.4) | 3(8.8) | ||
| 少许 | 54(57.4) | 27(79.4) | ||
| 丰富 | 34(36.2) | 4(11.8) |
注:*表示采用Fisher精确检验;#表示对有声晕病例进行分析;-表示无相应统计值。CDFI为彩色多普勒血流成像。钙化特征两两比较:无钙化vs 粗大钙化,P=0.009;无钙化vs 微钙化,P<0.001;微钙化vs 粗大钙化,P=0.004。CDFI特征两两比较:无血流vs 少许血流,P=0.633;无血流vs 丰富血流,P=0.117;少许血流vs 丰富血流,P=0.008 |
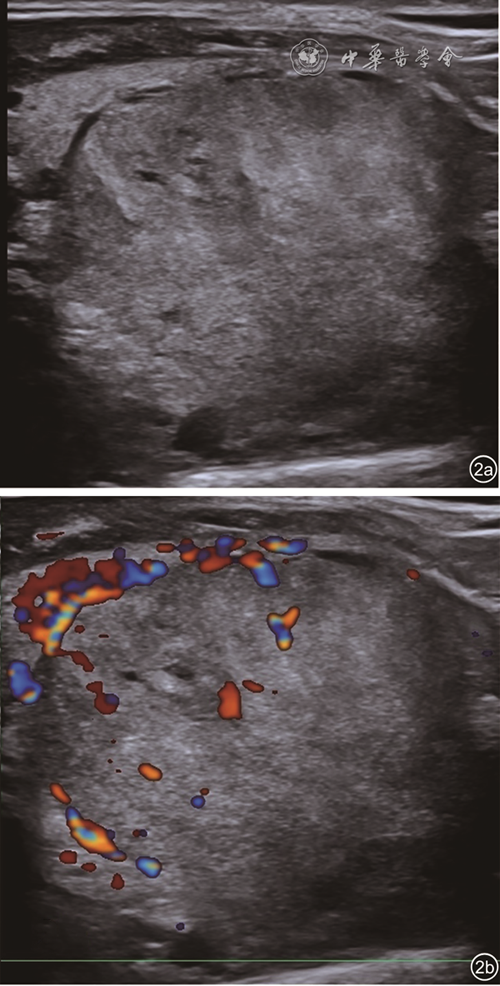
图1 女性患者,39岁,甲状腺左叶等回声结节,边缘光整,水平位生长,无钙化,声晕厚度一致,回声质地均匀(图a),彩色多普勒血流成像(图b)示内部少许血流,病理为结节性甲状腺肿 |
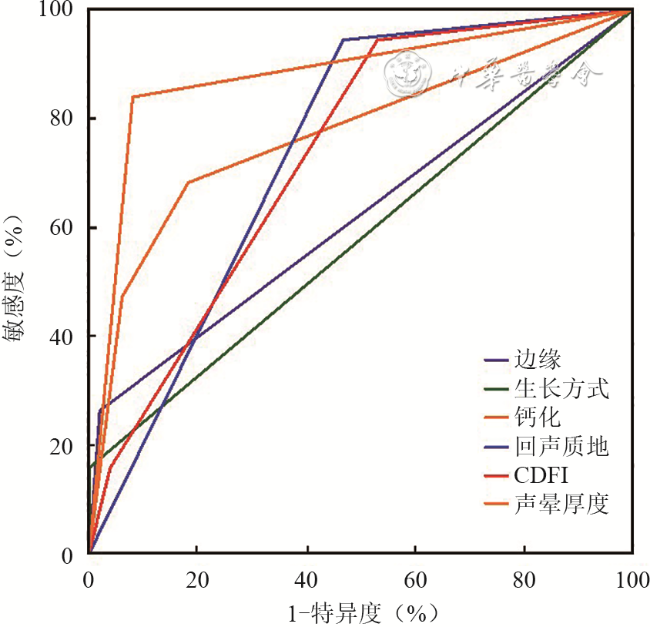
表3 甲状腺结节超声特征诊断结节良恶性的效能 |
| 超声特征 | 约登指数 | AUC | 敏感度(%) | 特异度(%) | 准确性(%) |
|---|---|---|---|---|---|
| 边缘 | 0.329 | 0.665 | 38.24 | 94.68 | 79.69 |
| 生长方式 | 0.155 | 0.578 | 17.65 | 97.87 | 76.56 |
| 钙化 | 0.565 | 0.803 | 73.53 | 82.98 | 80.47 |
| 回声质地 | 0.388 | 0.694 | 94.12 | 44.68 | 57.81 |
| CDFI | 0.244 | 0.622 | 88.24 | 36.17 | 51.26 |
| 声晕厚度 | 0.761 | 0.880 | 84.21 | 91.84 | 89.71 |
注:AUC为曲线下面积;CDFI为彩色多普勒血流成像 |
| 1 |
|
| 2 |
|
| 3 |
周建桥, 詹维伟. 2020年中国超声甲状腺影像报告和数据系统(C-TIRADS)指南解读 [J]. 诊断学理论与实践, 2020, 19(4): 350-353.
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
王帅, 徐辉雄, 徐军妹, 等. 甲状腺结节微钙化、粗大钙化及环状钙化与甲状腺癌的相关性分析 [J]. 影像诊断与介入放射学, 2015, 24(3): 212-215.
|
| 8 |
|
| 9 |
敬文莉, 王红, 王冬梅, 等. 对比甲状腺髓样癌与滤泡癌超声特征 [J]. 中国医学影像技术, 2020, 36(9): 1413-1415.
|
| 10 |
覃业志, 黄伟俊, 李凤, 等. 超声对甲状腺滤泡癌与滤泡腺瘤的鉴别诊断价值 [J]. 中国临床医学影像杂志, 2018, 29(8): 590-592.
|
| 11 |
庄玲玲. 声像图所示甲状腺恶性结节钙化特点与组织病理类型分析 [J]. 中国医学影像技术, 2019, 35(8): 1271-1273.
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
|
| 17 |
|
| 18 |
|
| 19 |
侯怡卿, 钱乐, 杨志芳, 等. 桥本甲状腺炎合并良恶性结节的超声特征比较分析 [J/OL]. 中华医学超声杂志(电子版), 2020,17(8): 742-747.
|
/
| 〈 |
|
〉 |




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}