
2023 , Vol. 20 >Issue 11: 1164 - 1173
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2023.11.010
多声学技术参数联合血清学指标对非酒精性脂肪性肝病肝脂肪变性阶段的诊断价值
Copy editor: 吴春凤
收稿日期: 2022-11-09
网络出版日期: 2024-01-15
基金资助
国家自然科学基金(82030048)
浙江省医药卫生科技计划项目(2023RC022)
版权
Value of multiple acoustic technical parameters combined with serological indicators in diagnosis of hepatic steatosis
Received date: 2022-11-09
Online published: 2024-01-15
Copyright
探讨多声学技术参数对非酒精性脂肪性肝病(NAFLD)脂肪变性阶段的诊断效能,并进一步探讨声学技术参数联合血清学参数是否能提高其诊断效能。
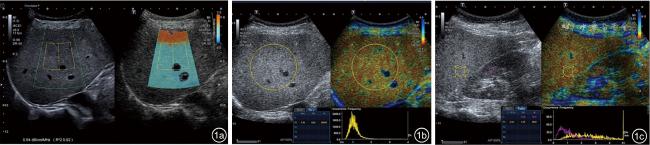
从2020年6月至2021年12月前瞻性连续入组在浙江大学医学院附属第二医院就诊的临床可疑NAFLD并行肝穿刺活检的病例。所有病例穿刺前均经过衰减成像(ATI)、归一化局部方差(NLV)、肝肾强度对比(Ratio)值等肝多声学技术参数检查,同时收集患者临床背景数据和血清学数据。以病理结果为金标准,采用Spearman秩相关分析评估多声学技术参数和临床参数与肝脂肪变性之间的相关性,绘制受试者操作特征曲线评价多声学技术参数对肝脂肪变性的诊断效能,并探索最佳声学技术参数与血清学参数联合是否能提高NAFLD肝脂肪变性的诊断效能。
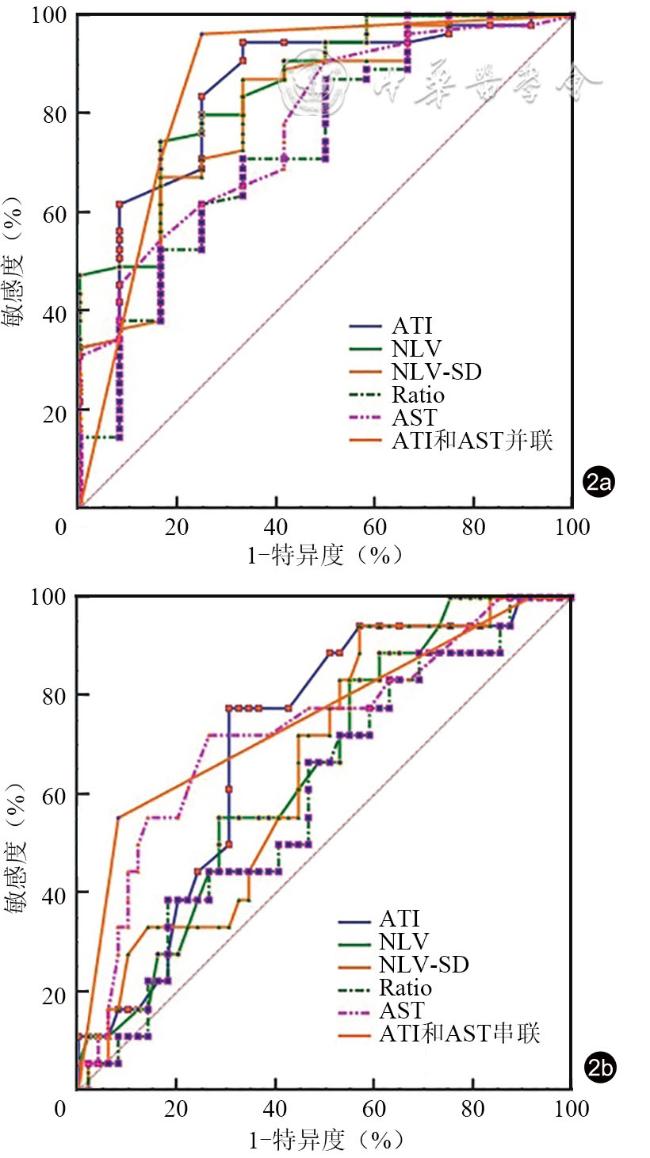
本研究共纳入病例75例,其中肝脂肪变性分级S0、S1、S2、S3级分别为15、41、13、6例。肝脂肪变性分级与声学技术参数衰减系数(AC)值、Ratio值呈显著正相关(相关系数r=0.519、0.285,P<0.001、=0.016),与声学技术参数NLV、NLV的标准差(NLV-SD)呈显著负相关(r=-0.391、-0.356,P=0.001、0.002)。当AC值<0.62 dB/(cm·MHz)或谷草转氨酶(AST)<18 IU/L时,ATI和AST并联诊断肝脂肪变性≥S1级的曲线下面积(AUC)为0.864(95%CI:0.765~0.933),其敏感度和特异度分别为91.5%、80.0%;当AC>0.75 dB/(cm·MHz)且AST>25 IU/L时,ATI和AST串联诊断肝脂肪变性≥S2级的AUC为0.761(95%CI:0.645~0.854),其敏感度和特异度分别为55.6%、92.5%。
在NAFLD患者中,声学技术参数AC、NLV、NLV-SD、Ratio值均在诊断肝脂肪变性分级中具有一定的价值。将AC值和血清学指标AST并联诊断可以进一步提高肝脂肪变性≥S1级的诊断效能,而AC值和AST串联诊断可以进一步提高肝脂肪变性≥S2级的诊断效能。
赵亚楠 , 方明 , 徐绍岩 , 魏树梅 , 张慧 , 黄奕宁 , 刘亚静 , 黄品同 . 多声学技术参数联合血清学指标对非酒精性脂肪性肝病肝脂肪变性阶段的诊断价值[J]. 中华医学超声杂志(电子版), 2023 , 20(11) : 1164 -1173 . DOI: 10.3877/cma.j.issn.1672-6448.2023.11.010
To investigate the diagnostic performance of multiple acoustic technical parameters for hepatic steatosis, an early stage of non-alcoholic fatty liver disease (NAFLD), and to further explore whether acoustic technical parameters combined with serological indicators can improve the diagnostic performance.
We prospectively enrolled 75 consecutive patients with suspected NAFLD who underwent percutaneous liver biopsy for evaluation of hepatic steatosis from June 2020 to December 2021. All cases underwent liver multiparametric ultrasound to obtain the acoustic technical parameters attenuation coefficient (AC), normalized local variance (NLV), and liver and kidney ratio (Ratio) before the liver biopsy procedure. The clinical data and serological data of the patients were collected at the same time. The correlation between the acoustic technical parameters and clinical indicators with hepatic steatosis was assessed by Spearman rank correlation, the diagnostic performance of the acoustic technical parameters for hepatic steatosis was assessed by receiver operating characteristic curve analysis, and the diagnostic performance of optimal acoustic technical parameters combined with serological indicators for hepatic steatosis was also analyzed.
A total of 75 cases were included in this study. The distribution of hepatic steatosis grades on histopathology was 15/41/13/6 for none (<5%, S0)/mild (5%-33%, S1)/moderate (>33%-66%, S2)/severe steatosis (>66%, S3), respectively. The AC value (r=0.519, P<0.001) and Ratio value (r=0.285, P=0.016) showed a significant positive correlation with hepatic steatosis, while the NLV value (r=-0.391, P=0.001) and NLV-SD value (r=-0.356, P=0.002) showed a significant negative correlation with hepatic steatosis. When AC<0.62 dB/(cm·MHz) or aspartate aminotransferase (AST) < 18 IU/L, the AUC of the parallel diagnosis of ATI and AST for the detection of hepatic steatosis≥S1 grade was 0.864 (95% confidence interval [CI]: 0.765-0.933), with a sensitivity of 91.5% and specificity of 80.0%. When AC>0.75dB/(cm·MHz) and AST>25 IU/L, the AUC of the tandem diagnosis of ATI and AST for the detection of hepatic steatosis ≥ S2 grade was 76.1% (95%CI: 0.645-0.854), with a sensitivity of 5.6% and specificity of 92.5%.
The acoustic technical parameters AC, NLV, NLV-SD, and Ratio have appreciated diagnostic performance in detecting varying degrees of hepatic steatosis in NAFLD patients. The parallel diagnosis of AC and AST can improve the diagnostic performance for hepatic steatosis≥S1 grade, while the tandem diagnosis of AC and AST can improve the diagnostic performance for hepatic steatosis≥S2 grade.
 表示,不符合正态分布的变量以M(QR)表示,计数资料以绝对值和百分数表示。采用Spearman秩相关分析评估病理脂肪变分级与各声学技术参数AC、NLV、NLV的标准差(standard deviation of NLV,NLV-SD)、Ratio及临床参数之间的相关性。各声学技术参数及临床参数在不同等级脂肪变之间差异比较应用秩和检验(Kruskal–Wallis检验)。以各病理参数及临床参数为自变量,以AC值、NLV值、NLV-SD值、Ratio值为应变量,行单因素和多因素回归分析,得出AC值、NLV值、NLV-SD值、Ratio值的显著影响因素。筛选出单因素分析时差异有统计学意义(P<0.05)的变量,以脂肪变性分级为应变量,行多元有序Logistics回归分析,得出脂肪变性的独立预测因素。不同指标及相关指标联合对肝脂肪变性的诊断效能应用受试者操作特征(receiver operator characteristic,ROC)曲线进行分析。以P<0.05为差异具有统计学意义。
表示,不符合正态分布的变量以M(QR)表示,计数资料以绝对值和百分数表示。采用Spearman秩相关分析评估病理脂肪变分级与各声学技术参数AC、NLV、NLV的标准差(standard deviation of NLV,NLV-SD)、Ratio及临床参数之间的相关性。各声学技术参数及临床参数在不同等级脂肪变之间差异比较应用秩和检验(Kruskal–Wallis检验)。以各病理参数及临床参数为自变量,以AC值、NLV值、NLV-SD值、Ratio值为应变量,行单因素和多因素回归分析,得出AC值、NLV值、NLV-SD值、Ratio值的显著影响因素。筛选出单因素分析时差异有统计学意义(P<0.05)的变量,以脂肪变性分级为应变量,行多元有序Logistics回归分析,得出脂肪变性的独立预测因素。不同指标及相关指标联合对肝脂肪变性的诊断效能应用受试者操作特征(receiver operator characteristic,ROC)曲线进行分析。以P<0.05为差异具有统计学意义。表1 75例可疑非酒精性脂肪性肝病患者一般临床资料 |
| 参数 | 数值 |
|---|---|
| 年龄[岁,M(QR)] | 54.0(40.0,60.0) |
| 性别(例,男/女) | 35/40 |
| 糖尿病病史(例) | 11 |
| 高血压病史(例) | 36 |
| 体质量指数[kg/m2,M(QR)] | 25.8(23.7,28.6) |
腰围(cm, ) ) | 94.5±10.0 |
| 肝生化 | |
| AST[IU/L,M(QR)] | 24.0(19.0,29.0) |
| ALT[IU/L,M(QR)] | 24.0(19.0,40.0) |
| GGT[IU/L,M(QR)] | 31.0(19.8,49.8) |
ALP(IU/L, ) ) | 84.4±24.1 |
| TBIL[μmol/L,M(QR)] | 12.9(9.1,15.2) |
| 脂相关指标 | |
TC(mmol/L, ) ) | 5.3±1.1 |
| HDL-C[mmol/L,M(QR)] | 1.2(1.0,1.3) |
LDL-C(mmol/L, ) ) | 3.0±0.7 |
| TG[mmol/L,M(QR)] | 1.8(1.3,2.3) |
ALB(g/dl, ) ) | 43.4±2.9 |
| 血小板计数[×109/L,M(QR)] | 213.0(180.8,257.8) |
| Glu(mmol/L,M(QR)] | 5.4(5.0,6.0) |
BUN(mmol/L, ) ) | 4.9±1.3 |
| 尿酸[μmol/L,M(QR)] | 344.0(300.0,442.5) |
| 皮肤距肝包膜距离[cm,M(QR)] | 1.8(1.6,2.1) |
| 脂肪变分级[例(%)] | |
| S0 | 15(20.0) |
| S1 | 41(54.7) |
| S2 | 13(17.3) |
| S3 | 6(8.0) |
| 小叶内炎症评分[例(%)] | |
| I0 | 30(40.0) |
| I1 | 36(48.0) |
| I2 | 7(9.3) |
| I3 | 2(2.7) |
| 气球样变评分[例(%)] | |
| 0分 | 59(78.7) |
| 1分 | 13(17.3) |
| 2分 | 3(4.0) |
| 纤维化分级[例(%)] | |
| F0期 | 48(64.0) |
| F1期 | 20(26.7) |
| F2期 | 6(8.0) |
| F3期 | 1(1.3) |
| F4期 | 0(0) |
注:AST为谷草转氨酶,ALT为谷丙转氨酶,GGT为谷氨酰转肽酶,ALP为碱性磷酸酶,TBIL为总胆红素,TC为总胆固醇,HDL-C为高密度脂蛋白胆固醇,LDL-C为低密度脂蛋白胆固醇,TG为甘油三酯,ALB为白蛋白,Glu为空腹血糖,BUN为血浆尿素氮 |
表2 肝脂肪变性病理分级与声学技术参数和临床参数的相关性 |
| 项目 | AC | NLV | NLV-SD | Ratio | 性别 | 年龄 | BMI | 高血压 | 糖尿病 | AST | ALT | 腰围 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| r值 | 0.519 | -0.391 | -0.356 | 0.285 | -0.159 | 0.175 | 0.188 | 0.003 | 0.023 | 0.450 | 0.520 | 0.225 |
| P值 | <0.001 | 0.001 | 0.002 | 0.016 | 0.173 | 0.132 | 0.106 | 0.981 | 0.844 | <0.001 | <0.001 | 0.095 |
| 项目 | TG | TC | GGT | TBIL | ALP | ALB | LDL-C | HDL-C | BUN | 尿酸 | 皮肤距肝包膜距离 | |
| r值 | -0.175 | 0.017 | 0.301 | 0.255 | 0.066 | 0.280 | -0.035 | 0.096 | -0.233 | 0.018 | 0.279 | |
| P值 | 0.134 | 0.882 | 0.009 | 0.027 | 0.064 | 0.015 | 0.767 | 0.411 | 0.044 | 0.882 | 0.015 |
注:AC为衰减系数,NLV为归一化局部方差,NLV-SD为归一化局部方差的标准差,Ratio为肝肾强度比值,BMI为体质量指数,AST为谷草转氨酶,ALT为谷丙转氨酶,TG为甘油三酯,TC为总胆固醇,GGT为谷氨酰转肽酶,TBIL为总胆红素,ALP为碱性磷酸酶,ALB为白蛋白,LDL-C为低密度脂蛋白胆固醇,HDL-C为高密度脂蛋白胆固醇,BUN为血浆尿素氮 |
表3 声学技术参数及临床参数在不同级别肝脂肪变性中的差异比较 |
| 参数 | S0(n=15) | S1(n=41) | ≥S2(n=19) | Z值 | P值 |
|---|---|---|---|---|---|
AC[dB/(cm·MHz), ] ] | 0.63±0.07 | 0.75±0.12 | 0.82±0.12 | 20.389 | <0.001 |
NLV( ) ) | 1.35±0.28 | 1.11±0.08 | 1.08±0.06 | 14.659 | 0.001 |
NLV-SD( ) ) | 0.82±0.57 | 0.41±0.24 | 0.33±0.13 | 11.188 | 0.004 |
Ratio( ) ) | 1.55±0.78 | 2.34±1.08 | 2.46±1.08 | 7.612 | 0.022 |
| 年龄[岁,M(QR)] | 52(33,57) | 54(44,59) | 55(39,67) | 2.865 | 0.239 |
| BMI[kg/m2,M(QR)] | 25.1(23.0,29.4) | 25.8(23.5,28.3) | 27.2(24.4,30.9) | 2.950 | 0.229 |
腰围(cm, ) ) | 91.5±12.0 | 93.6±10.3 | 98.0±7.5 | 3.603 | 0.165 |
| AST[IU/L,M(QR)] | 18.0(15.0,23.0) | 24.0(19,28) | 30.0(26.0,71.0) | 15.563 | <0.001 |
| ALT[IU/L,M(QR)] | 21.0(11.0,23.0) | 23.0(19.0,40.5) | 37.0(26.0,71.0) | 20.038 | <0.001 |
| Glu[mg/dl,M(QR)] | 4.93(4.61,6.00) | 5.42(5.10,6.11) | 5.52(5.10,5.75) | 2.482 | 0.289 |
| TG[mg/dl,M(QR)] | 2.1(1.5,2.3) | 1.7(1.3,2.3) | 1.5(1.3,2.7) | 2.291 | 0.318 |
TC(mg/dl, ) ) | 5.41±0.85 | 5.27±1.24 | 5.40±1.05 | 1.191 | 0.551 |
| GGT[IU/L,M(QR)] | 20.0(16.0,31.0) | 31.0(20.5,53.0) | 41.5(22.5,73.3) | 7.127 | 0.028 |
| TBIL[μmol/L,M(QR)] | 11.0(7.5,14.5) | 11.7(9.1,15.7) | 14.2(12.8,16.1) | 4.804 | 0.091 |
ALP(IU/L, ) ) | 85.2±34.9 | 83.2±20.5 | 86.2±22.4 | 0.438 | 0.803 |
ALB(g/dl, ) ) | 41.5±2.1 | 43.9±3.0 | 43.9±2.9 | 9.901 | 0.007 |
LDL-C(mg/dl, ) ) | 3.09±0.56 | 2.90±0.78 | 2.97±0.70 | 1.323 | 0.516 |
| HDL-C[mg/dl,M(QR)] | 1.16(1.00,1.30) | 1.1(1.01,1.37) | 1.20(1.00,1.40) | 0.759 | 0.684 |
BUN(mmol/L, ) ) | 5.42±0.82 | 4.79±1.40 | 4.59±1.17 | 5.117 | 0.077 |
| 尿酸[μmol/L,M(QR)] | 344.0(277.0,444.0) | 342.0(302.5,446.5) | 345.5(300.3,435.3) | 0.023 | 0.988 |
| 皮肤距肝包膜距离[cm,M(QR)] | 1.7(1.5,2.1) | 1.8(1.6,2.1) | 1.9(1.7,2.2) | 5.989 | 0.050 |
注:AC为衰减系数,NLV为归一化局部方差,NLV-SD为归一化局部方差的标准差,Ratio为肝肾强度比值,BMI为体质量指数,AST为谷草转氨酶,ALT为谷丙转氨酶,Glu为空腹血糖,TG为甘油三酯,TC为总胆固醇,GGT为谷氨酰转肽酶,TBIL为总胆红素,ALP为碱性磷酸酶,ALB为白蛋白,LDL-C为低密度脂蛋白胆固醇,HDL-C为高密度脂蛋白胆固醇,BUN为血浆尿素氮 |
表4 AC、NLV、NLV-SD、Ratio值诊断不同级别肝脂肪变性的诊断效能 |
| 参数 | 脂肪变性分级 | 截断值 | AUC(95%CI) | SE[%(95%CI)] | SP[%(95%CI)] | PPV[%(95%CI)] | NPV[%(95%CI)] |
|---|---|---|---|---|---|---|---|
| AC | S0 vs S1,≥S2 | >0.62 | 0.852(0.748~0.925) | 92.9(82.7~98.0) | 66.7(38.4~88.2) | 54.4(36.8~71.0) | 95.6(88.8~98.4) |
| S0,S1 vs ≥S2 | >0.75 | 0.731(0.613~0.830) | 77.8(52.4~93.6) | 71.7(57.7~83.2) | 54.1(41.8~65.9) | 88.3(75.7~94.8) | |
| NLV | S0 vs S1,≥S2 | <1.14 | 0.845(0.739~0.920) | 72.9(59.7~83.6) | 83.3(51.6~97.9) | 65.2(34.4~87.0) | 87.8(81.5~92.1) |
| S0,S1 vs ≥S2 | ≤1.18 | 0.639(0.516~0.750) | 100(82.4~100) | 25.0(14.0~38.9) | 36.4(32.8~40.1) | 100(100~100) | |
| NLV-SD | S0 vs S1,≥S2 | ≤0.56 | 0.795(0.683~0.882) | 86.4(75.0~94.0) | 66.7(34.9~90.1) | 52.6(33.2~71.3) | 92.0(84.3~96.1) |
| S0,S1 vs ≥S2 | ≤0.49 | 0.639(0.516~0.750) | 94.7(74.0~99.9) | 42.3(28.7~56.8) | 41.3(35.3~47.6) | 94.9(73.1~99.2) | |
| Ratio | S0 vs S1,≥S2 | >1.58 | 0.748(0.631~0.843) | 72.9(59.7~83.6) | 66.7(34.9~90.1) | 48.4(29.3~67.9) | 85.2(76.3~91.1) |
| S0,S1 vs ≥S2 | >2.75 | 0.603(0.480~0.717) | 42.1(20.3~66.5) | 80.8(67.5~90.4) | 48.4(30.4~66.9) | 76.5(68.4~83.0) |
注:AC为衰减系数,NLV为归一化局部方差,NLV-SD为归一化局部方差的标准差,Ratio为肝肾强度比值,AUC为曲线下面积,SE为敏感度,SP为特异度,PPV为阳性预测值,NPV为阴性预测值,CI为可信区间 |
表5 AC值联合AST对肝脂肪变性的联合诊断效能 |
| 参数 | 脂肪变性分级 | 截断值 | AUC(95%CI) | SE[%(95%CI)] | SP[%(95%CI)] | PPV[%(95%CI)] | NPV[%(95%CI)] |
|---|---|---|---|---|---|---|---|
| AC | S0 vs S1,≥S2 | >0.62 | 0.852(0.748~0.925) | 92.9(82.7~98.0) | 66.7(38.4~88.2) | 54.4(36.8~71.0) | 95.6(88.8~98.4) |
| S0,S1 vs ≥S2 | >0.75 | 0.731(0.613~0.830) | 77.8(52.4~93.6) | 71.7(57.7~83.2) | 54.1(41.8~65.9) | 88.3(75.7~94.8) | |
| AST | S0 vs S1,≥S2 | >18 | 0.789(0.680~0.875) | 88.3(77.4~95.2) | 53.3(26.6~78.7) | 44.8(31.9~58.4) | 91.4(82.1~96.1) |
| S0,S1 vs ≥S2 | >25 | 0.718(0.602~0.816) | 68.4(43.4~87.4) | 75.0(61.6~85.6) | 54.0(40.4~67.0) | 84.7(73.8~91.6) | |
| AC+AST | S0 vs S1,≥S2 | AC<0.62或AST<18 | 0.864(0.765~0.933) | 91.5(81.3~97.2) | 80.0(51.9~95.7) | 66.2(41.5~84.4) | 95.7(90.0~98.1) |
| S0,S1 vs ≥S2 | AC>0.75且AST>25 | 0.761(0.645~0.854) | 55.6(30.8~78.5) | 92.5(81.8~97.9) | 75.9(53.0~89.8) | 82.9(74.2~89.1) |
注:AC为衰减系数,AST为谷草转氨酶,AUC为曲线下面积,SE为敏感度,SP为特异度,PPV为阳性预测值,NPV为阴性预测值,CI为可信区间 |
| 1 |
European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease [J]. J Hepatol, 2016, 64(6): 1388-1402.
|
| 2 |
|
| 3 |
|
| 4 |
|
| 5 |
|
| 6 |
|
| 7 |
|
| 8 |
|
| 9 |
包静文, 朱宇莉, 徐庆玥, 等. 超声声衰减成像评估代谢相关脂肪性肝病肝脂肪变程度的应用价值 [J]. 中华超声影像学杂志, 2021, 30(10): 868-873.
|
| 10 |
|
| 11 |
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
张馨悦, 孝梦甦, 吕珂, 等. 非酒精性脂肪性肝病的超声评价方法及应用现状 [J]. 中华健康管理学杂志, 2021, 15(1): 83-86.
|
| 16 |
|
| 17 |
|
| 18 |
赵亚楠, 黄品同. 超声相关技术在诊断非酒精性脂肪性肝病中的研究进展 [J/OL]. 中华医学超声杂志(电子版), 2022, 19(3): 272-276.
|
| 19 |
陈洁, 张波. 超声定量评估非酒精性脂肪肝病肝脏脂肪变性的研究进展 [J]. 中国医学科学院学报, 2021, 43(5): 827-832.
|
| 20 |
|
| 21 |
|
| 22 |
|
| 23 |
|
| 24 |
姚明解, 文夏杰, 王雷婕, 等. 基于瞬时弹性成像技术检测参数的非酒精性脂肪性肝病 进展评估模型的建立 [J]. 临床肝胆病杂志, 2021, 37(7): 1614-1618.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}