
2024 , Vol. 21 >Issue 03: 268 - 274
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2024.03.004
超声O-RADS分类和临床特征对不同病理类型卵巢浆液性肿瘤的诊断价值
Copy editor: 吴春凤
收稿日期: 2023-02-03
网络出版日期: 2024-06-05
基金资助
浙江省自然科学基金(LQ20H180011)
版权
Value of ultrasound O-RADS classification and clinical characteristics in diagnosis of ovarian serous tumors of different pathological types
Received date: 2023-02-03
Online published: 2024-06-05
Copyright
探讨卵巢浆液性肿瘤不同病理类型之间的卵巢-附件影像报告和数据系统(O-RADS)超声特征及临床特征的差异,并分析超声O-RADS分类和临床特征在诊断不同病理类型卵巢浆液性肿瘤方面的应用价值。
回顾性分析2021年1月至2022年6月浙江大学医学院附属第二医院经病理证实为卵巢浆液性肿瘤的病例57例,共76个附件肿块,记录患者的临床资料及超声图像。依据组织病理学类型将卵巢浆液性肿瘤患者分为良性肿瘤组(20例)、交界性肿瘤组(16例)和恶性肿瘤组(21例)。采用单因素方差分析3组患者年龄、体质量指数及肿瘤最大径的差异;采用秩和检验对3组患者糖类抗原125(CA125)水平、病灶血流评分、病灶内乳头状突起数目及病灶O-RADS分类进行两两比较;采用χ2检验分析3组患者主诉的差异;采用Bonferroni χ2分割法对患者是否合并有腹水和(或)腹膜增厚/结节、病变发生部位、病灶性质、病灶内有无分隔进行两两比较;绘制受试者操作特征(ROC)曲线评价CA125、O-RADS分类对卵巢浆液性肿瘤的诊断效能。
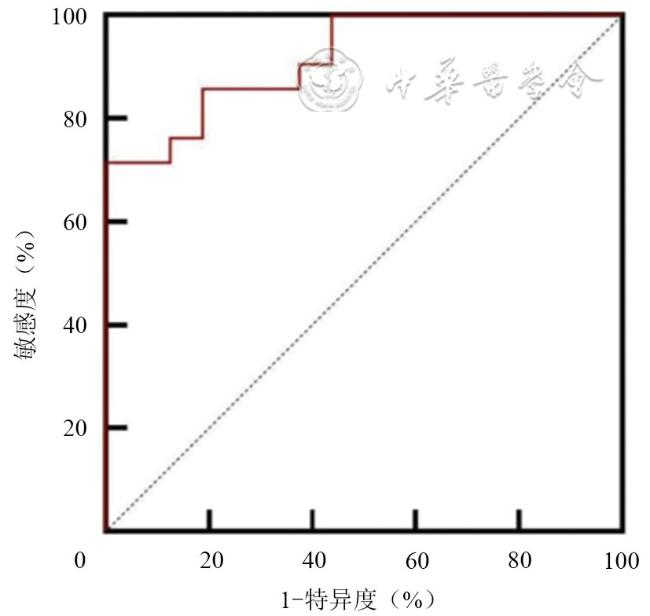
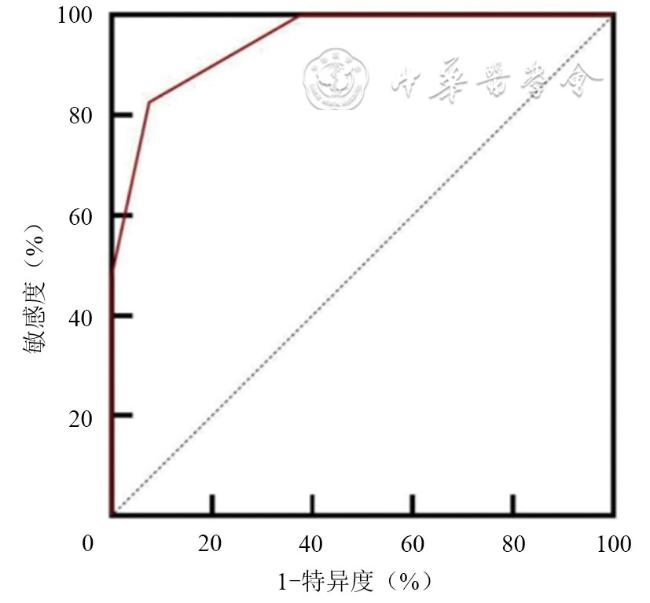
临床特征上,良性肿瘤组、交界性肿瘤组和恶性肿瘤组病变位于双侧[15.0%(3/20)vs 18.7%(3/16)vs 61.9%(13/21)]、合并出现腹水和(或)腹膜增厚/结节[0%(0/20)vs 0%(0/16)vs 57.1%(12/21)]及血清CA125水平[15.8(7.8,21.7)U/ml vs 43.3(29.4,105.6)U/ml vs 1229.2(142.9,2222.7)U/ml]比较,差异具有统计学意义(χ2=12.271,P=0.003;χ2=18.321,P<0.001;H=38.393,P<0.001),血清CA125水平截断值为293.0 U/ml(曲线下面积=0.917),诊断恶性肿瘤的敏感度为71.43%,特异度为100%。超声特征方面,良性肿瘤组、交界性肿瘤组和恶性肿瘤组病变呈多房囊性含实性成分及实性/实性样变[13.1%(3/23)vs 21.0%(4/19)vs 91.2%(31/34)]、病灶血流评分≥2分[0%(0/23)vs 68.4%(13/19)vs 82.4%(28/34)]、囊性病灶内含乳头状数目>3个[0%(0/23)vs 68.4%(13/19)vs 8.7%(2/23)]、囊性病灶呈多房[34.8%(8/23)vs 21.1%(4/19)vs 87.0%(20/23)]比较,差异具有统计学意义(χ2=89.998,P<0.001;H=35.407,P<0.001;H=26.210,P<0.001;χ2=19.477,P<0.001)。ROC曲线分析显示,O-RADS 4-5类诊断交界性肿瘤或恶性浆液性肿瘤的敏感度为92.45%,特异度为82.61%。
不同病理类型的卵巢浆液性肿瘤具有不同的超声特征及临床特征,超声O-RADS分类(病灶性质、病灶内有无分隔、病灶血流评分、病灶内乳头状突起数目)和临床特征(患者CA125水平、病变部位)可有效区分不同病理类型的卵巢浆液性肿瘤。
关键词: 卵巢浆液性肿瘤; 超声; 卵巢-附件影像报告和数据系统; 临床特征
张焱 , 刘春媚 , 姚瑾 , 陈苗苗 , 徐雯 , 黄品同 . 超声O-RADS分类和临床特征对不同病理类型卵巢浆液性肿瘤的诊断价值[J]. 中华医学超声杂志(电子版), 2024 , 21(03) : 268 -274 . DOI: 10.3877/cma.j.issn.1672-6448.2024.03.004
To investigate the differences in ultrasound features according to the ovarian-adnexal reporting and data system (O-RADS) and clinical characteristics among ovarian serous tumors of different pathological types, and to analyze the application value of ultrasonic O-RADS characteristics and clinical characteristics in the diagnosis of ovarian serous tumors of different pathological types.
A total of 57 patients diagnosed with ovarian serous tumors, containing 76 adnexal masses, by pathological examination at The Second Affiliated Hospital of Zhejiang University School of Medicine from January 2021 to June 2022 were retrospectively analyzed. The clinical data and ultrasound images of the patients were recorded. The patients were divided into benign serous tumor group (n=20), serous borderline tumor group (n=16), and malignant serous tumor (serous carcinoma) group (n=21) according to the histopathological type. One-way analysis of variance was used to compare the differences in age, body mass index, and maximum tumor diameter among patients of the three groups. The rank sum test was used to compare the CA125 level, blood flow, number of papillary projections, and O-RADS characteristics between any two groups of the three groups. The chi-square test was used to analyze the differences in chief complaints among patients of the three groups. The chi-square test with Bonferroni correction was used to compare peritoneal thickening/nodules and (or) abdominal effusion, lesion location, composition, and complete separation between any two groups of the three groups. Receiver operating characteristic curve (ROC) analysis was used to assess the diagnostic performance of CA125 and O-RADS classification for ovarian serous tumors.
In terms of clinical characteristics, the percentage of bilateral lesions in the benign, borderline, and malignant tumor groups was 15.0% (3/20) vs 18.7% (3/16) vs 61.9% (13/21), the percentage of patients accompanied by peritoneal thickening/nodules and (or) abdominal effusion was 0% (0/20) vs 0% (0/16) vs 57.1% (12/21), and the percentage of patients with high serum CA125 levels was 15.8 (7.8, 21.7) U/ml vs 43.3 (29.4, 105.6) U/ml vs 1229.2 (142.9, 2222.7) U/ml; the differences among the three groups were statistically significant (χ2=12.271, P=0.003; χ2=18.321, P<0.001; H=38.393, P<0.001). The cut-off value of serum CA125 level for diagnosing malignant serous tumors was 293.0 U/ml (area under the curve [AUC]=0.917), with a sensitivity and specificity of 71.43% and 100%, respectively. In terms of ultrasound features, the percentage of multilocular cyst lesions with solid component(s) in the benign, borderline, and malignant tumors groups was 13.1% (3/23) vs 21.0% (4/19) vs 91.2% (31/34), the percentage of lesions with blood flow score ≥2 was 0% (0/23) vs 68.4% (13/19) vs 82.4% (28/34), the percentage of cystic lesions with the number of papillary projections >3 was 0% (0/23) vs 68.4% (13/19) vs 8.7% (2/23), and the percentage of multilocular cystic lesions was 34.8% (8/23) vs 21.1% (4/19) vs 87.0% (20/23); the differences were statistically significant among the three groups (χ2=89.998, P<0.001; H=35.407, P<0.001; H=26.210, P<0.001; χ2=19.477, P<0.001). The sensitivity and specificity of O-RADS 4-5 in diagnosing borderline or malignant serous tumors were 92.45% and 82.61%, respectively.
There are different ultrasonic O-RADS characteristics and clinical characteristics in ovarian serous tumors of different pathological types. They can be effectively distinguished by the clinical characteristics (CA125 level and lesion location) and ultrasonic O-RADS characteristics (composition, complete separation, blood flow, and number of papillary projections ) of the patients.
 表示,如呈非正态分布,则用M(QR)表示;计数资料和等级资料则采用频数和率表示;具有正态性及方差齐性的3组计量资料(年龄、体质量质数、肿瘤最大径)的差异比较采用单因素方差分析;不具有正态性的3组计量资料(CA125)及等级资料(病灶血流评分、病灶内乳头状突起数目、病灶O-RADS分类)的差异比较采用H检验,组间两两比较采用秩和检验;3组计数资料的差异比较采用χ2检验,组间(患者是否合并有腹水和(或)腹膜增厚/结节、病变发生部位、病灶性质、病灶内有无分隔)两两比较采用Bonferroni χ2分割法;受试者操作特征(receiver operating characteristic,ROC)曲线计算CA125、O-RADS分类曲线下面积(area under the curve,AUC)鉴别不同病理类型浆液性肿瘤的截断值、敏感度和特异度。以P<0.05为差异具有统计学意义。
表示,如呈非正态分布,则用M(QR)表示;计数资料和等级资料则采用频数和率表示;具有正态性及方差齐性的3组计量资料(年龄、体质量质数、肿瘤最大径)的差异比较采用单因素方差分析;不具有正态性的3组计量资料(CA125)及等级资料(病灶血流评分、病灶内乳头状突起数目、病灶O-RADS分类)的差异比较采用H检验,组间两两比较采用秩和检验;3组计数资料的差异比较采用χ2检验,组间(患者是否合并有腹水和(或)腹膜增厚/结节、病变发生部位、病灶性质、病灶内有无分隔)两两比较采用Bonferroni χ2分割法;受试者操作特征(receiver operating characteristic,ROC)曲线计算CA125、O-RADS分类曲线下面积(area under the curve,AUC)鉴别不同病理类型浆液性肿瘤的截断值、敏感度和特异度。以P<0.05为差异具有统计学意义。表1 卵巢浆液性恶性肿瘤组、交界性肿瘤组及良性肿瘤组的临床资料比较 |
| 临床资料 | 良性肿瘤组(n=20例) | 交界性肿瘤组(n=16例) | 恶性肿瘤组(n=21例) | 统计值 | P值 |
|---|---|---|---|---|---|
年龄(岁, ) ) | 51.05±15.33 | 50.13±14.39 | 54.14±12.14 | F=0.438 | 0.648 |
| 绝经[例(%)] | 10(50.0) | 7(43.8) | 12(57.1) | χ2=0.661 | 0.711 |
体质量指数(kg/m2, ) ) | 21.78±1.86 | 22.52±2.85 | 22.66±2.67 | F=0.477 | 0.624 |
| 主诉[例(%)] | χ2=6.304 | 0.382 | |||
| 体检发现(肿瘤标志物升高/盆腔肿块) | 13(65.0) | 12(75.0) | 9(42.9) | ||
| 月经不规律 | 1(5.0) | 0(0) | 2(9.5) | ||
| 绝经后阴道出血 | 2(10.0) | 1(6.3) | 1(4.7) | ||
| 腹痛/腹胀 | 4(20.0) | 3(18.7) | 9(42.9) | ||
肿瘤最大直径(cm, ) ) | 7.50±3.42 | 9.69±4.51 | 7.63±4.39 | F=2.548 | 0.085 |
| 血清CA125[U/ml,M(QR)] | 15.8(7.8,21.7) | 43.3(29.4,105.6)a | 1229.2(142.9,2222.7)ab | H=38.393 | <0.001 |
| 部位[例(%)] | χ2=12.271 | 0.003 | |||
| 单侧 | 17(85.0) | 13(81.3) | 8(38.1) | ||
| 双侧 | 3(15.0) | 3(18.7) | 13(61.9)ab | ||
| 腹水和(或)腹膜增厚/结节[例(%)] | 0(0) | 0(0) | 12(57.1)ab | χ2=18.321 | <0.001 |
注:CA125为糖类抗原125;a与良性肿瘤组比较,b与交界性肿瘤组比较,差异具有统计学意义(P<0.05) |
表2 卵巢浆液性恶性肿瘤组、交界性肿瘤组及良性肿瘤组的超声O-RADS分类比较[个(%)] |
| 分组 | 肿块数(个) | O-RADS分类 | ||
|---|---|---|---|---|
| ≤3类 | 4类 | 5类 | ||
| 良性肿瘤组 | 23 | 19(82.6) | 4(17.4) | 0(0) |
| 交界性肿瘤组a | 19 | 0(0) | 6(31.6) | 13(68.4) |
| 恶性肿瘤组b | 34 | 4(11.8) | 10(29.4) | 20(58.8) |
| 非良性肿瘤组c | 53 | 4(7.5) | 16(30.2) | 33(62.3) |
注:O-RADS为卵巢-附件影像报告和数据系统,非良性肿瘤组为交界性肿瘤组+恶性肿瘤组;a与良性肿瘤组比较,差异具有统计学意义(Z=-5.404,P<0.001),b与良性肿瘤组比较,差异具有统计学意义(Z=-5.713,P<0.001),a与b比较,差异无统计学意义(Z=-0.933,P=0.367),c与良性肿瘤组比较,差异具有统计学意义(Z=-6.337,P<0.001) |
表3 卵巢浆液性恶性肿瘤组、交界性肿瘤组及良性肿瘤组的超声特征比较[个(%)] |
| 组别 | 个数 | 性质 | 有无分隔 | |||||
|---|---|---|---|---|---|---|---|---|
| 单房囊性不含实性成分 | 多房囊性不含实性成分 | 单房囊性含实性成分 | 多房囊性含实性成分 | 实性或实性样病变 | 单房 | 多房 | ||
| 良性肿瘤组 | 23 | 14(60.9) | 5(21.7) | 1(4.3) | 3(13.1) | 0(0) | 15(65.2) | 8(34.8) |
| 交界性肿瘤组 | 19 | 1(5.3) | 0(0) | 14(73.7) | 4(21.0) | 0(0) | 15(78.9) | 4(21.1) |
| 恶性肿瘤组 | 34 | 0(0) | 0(0) | 3(8.8) | 20(58.8) | 11(32.4) | 3(13.0)* | 20(87.0)* |
| χ2值a | 27.545 | 0.961 | ||||||
| P值a | <0.001 | 0.495 | ||||||
| χ2值b | 43.046 | 12.768 | ||||||
| P值b | <0.001 | 0.001 | ||||||
| χ2值c | 27.763 | 17.578 | ||||||
| P值c | <0.001 | <0.001 | ||||||
| 组别 | 个数 | 乳头状突起数目 | 内部血流评分 | |||||
| 0个 | 1~3个 | >3个 | 1分 | 2分 | 3分 | 4分 | ||
| 良性肿瘤组 | 23 | 19(82.6) | 4(17.4) | 0(0) | 23(100) | 0(0) | 0(0) | 0(0) |
| 交界性肿瘤组 | 19 | 4(21.1) | 2(10.5) | 13(68.4) | 6(31.6) | 10(52.6) | 3(15.8) | 0(0) |
| 恶性肿瘤组 | 34 | 18(78.3)* | 3(13.0)* | 2(8.7)* | 6(17.6) | 15(44.1) | 10(29.5) | 3(8.8) |
| Z值a | -4.524 | -4.660 | ||||||
| P值a | <0.001 | <0.001 | ||||||
| Z值b | -0.492 | -5.698 | ||||||
| P值b | 0.609 | <0.001 | ||||||
| Z值c | -4.002 | -1.831 | ||||||
| P值c | <0.001 | 0.075 | ||||||
注:3组病灶性质、有无分隔、乳头状突起数目、内部血流评分比较,差异具有统计学意义(χ2=89.998,P<0.001;χ2=19.477,P<0.001,H=26.210,P<0.001;H=35.407,P<0.001);a为交界性肿瘤组与良性肿瘤组比较的结果,b为恶性肿瘤组与良性肿瘤组比较的结果,c为恶性肿瘤组与交界性肿瘤组比较的结果;*乳头状突起和有无分隔仅存在于囊性病灶,包括单房囊性不含实性成分、多房囊性不含实性成分、单房囊性含实性成分、多房囊性含实性成分病灶,恶性肿瘤组共计23个囊性病灶,百分率计算分母为23 |
| 1 |
WHO Classification of Tumours Editorial Board. WHO classification of tumours: female genital tumours [M]. Lyon (France): IARC Publications, 2020: 1‐632.
|
| 2 |
|
| 3 |
王青娟, 梁茜, 郑剑, 等. 超声造影联合卵巢-附件超声报告和数据风险分层系统的临床应用价值 [J]. 中华超声影像学杂志, 2022, 31(3): 220-225.
|
| 4 |
陈程, 戴晴. 美国放射学会卵巢-附件影像报告和数据系统超声风险分层与管理共识指南的解读[J/OL]. 中华医学超声杂志(电子版), 2020, 17(11): 1051-1060.
|
| 5 |
张丹, 王茜, 王佳颖. IOTA共识与O-RADS共识指南的解读与分析[J/OL]. 中华医学超声杂志(电子版), 2022, 19(2): 105-113.
|
| 6 |
|
| 7 |
|
| 8 |
|
| 9 |
|
| 10 |
|
| 11 |
漆玖玲, 陆蓓蕾, 樊韵玲, 等. 卵巢浆液性交界性肿瘤与卵巢浆液性囊腺瘤超声特征对比分析 [J]. 中国超声医学杂志, 2020, 36(10): 934-937.
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
张曼, 吴曼丽, 曲恩泽, 等. 超声卵巢-附件报告和数据系统评估附件肿物风险等级的重复性研究 [J]. 中华超声影像学杂志, 2022, 31(9): 797-801.
|
| 16 |
李晏杰, 朱熠, 张国楠. 卵巢-附件影像报告和数据系统(O-RADS)研究进展 [J]. 肿瘤预防与治疗, 2022, 35(5): 462-468.
|
| 17 |
甘雅端, 吕国荣, 杨舒萍, 等. 卵巢上皮性肿瘤超声鉴别特征及预测模型 [J]. 中华超声影像学杂志, 2020, 29(6): 534-539.
|
/
| 〈 |
|
〉 |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}