
2025 , Vol. 22 >Issue 04: 348 - 353
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.04.010
基于排泄性尿路超声造影诊断肾内反流及与DMSA 显像的相关性分析
Copy editor: 汪荣
收稿日期: 2025-03-05
网络出版日期: 2025-06-09
版权
Contrast-enhanced voiding urosonography-based assessment of intrarenal reflux: spatial correlation of intrarenal reflux with DMSA scintigraphy findings
Received date: 2025-03-05
Online published: 2025-06-09
Copyright
目的
探讨排泄性尿路超声造影(ceVUS)检测肾内反流(IRR)的临床价值及IRR 与放射性核素肾静态显像(DMSA)所示肾实质损伤部位的相关性。
方法
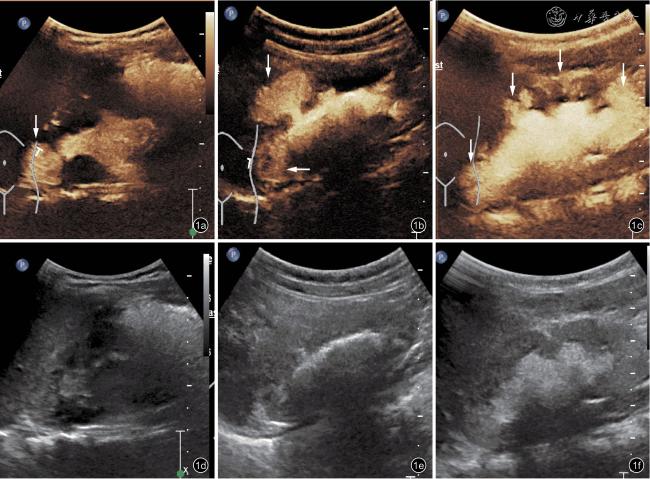
选取2021 年1 月至2024 年12 月在浙江大学医学院附属儿童医院经ceVUS 诊断为膀胱输尿管反流(VUR)的患者205 例[共410个肾盂-输尿管单位(PUUs)],其中302 个PUUs 存在不同程度的VUR。将肾实质内的集合小管内出现造影剂渗入定义为IRR。按肾脏长轴三等分法定位IRR 区域(上、中、下部)。比较不同VUR 级别及年龄组间IRR 检出率差异,并通过Kendall 相关性检验分析98 例(196 个PUUs)患儿的DMSA 显像异常部位与IRR 分布部位的空间一致性。
结果
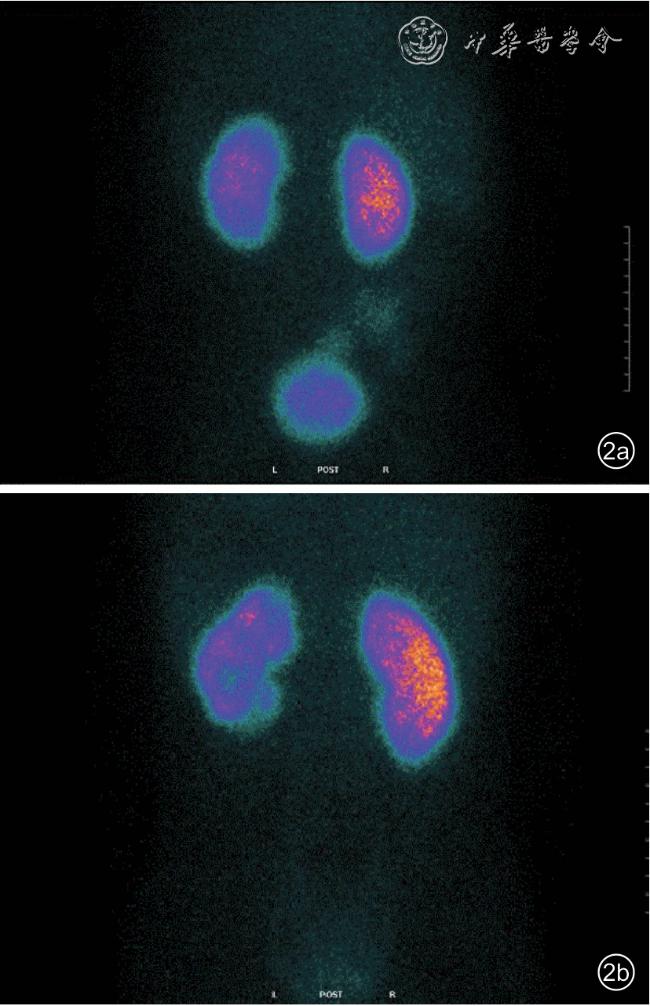
IRR 总检出率为20.86%(63/302),均见于Ⅲ级及以上的VUR 病例。不同VUR 分级的检出率分别为:Ⅲ级27.08%(26/96),Ⅳ级43.55%(27/62),V 级52.63%(10/19)。1 岁以下患儿IRR 发生率显著高于1 岁以上组[27.28%(35/126) vs 15.91%(28/176),P<0.05]。IRR 在肾脏的区域分布为:上部42.06%(53/126)、下部33.33%(42/126)、中部24.60%(31/126)。98 例(196 个PUUs)患儿的DMSA 显像异常发生率为51.53%(101/196),存在IRR 组的发生率高于无IRR 组[80.00%(44/55) vs 40.42%(57/141),P<0.05]。DMSA 异常在肾脏的区域分布为:上部47.78%(75/157)、下部36.94%(58/157)、中部15.29%(24/157);IRR 在肾脏的区域分布为:上部44.82%(39/87)、下部32.18%(28/87)、中部22.99%(20/87)。IRR 与DMSA 异常的部位呈中度程度相关(Kendall 相关系数0.543,P<0.05)。
结论
ceVUS 可有效识别Ⅲ级及以上VUR 患儿的IRR。IRR 发生与低龄及高反流级别相关。IRR 在肾脏的部位与DMSA 显像异常部位存在空间一致性,提示应将其纳入VUR 分级系统以优化临床决策。
杨秀珍 , 李丽 , 徐哲明 , 王晶晶 , 叶菁菁 . 基于排泄性尿路超声造影诊断肾内反流及与DMSA 显像的相关性分析[J]. 中华医学超声杂志(电子版), 2025 , 22(04) : 348 -353 . DOI: 10.3877/cma.j.issn.1672-6448.2025.04.010
Objective
s To investigate the clinical utility of contrast-enhanced voiding urosonography (ceVUS) in detecting intrarenal reflux (IRR) and analyze its spatial correlation with renal parenchymal damage identified by dimercaptosuccinic acid (DMSA) scintigraphy.
Methods
A cohort of 205 non-duplex kidney patients, 410 pyeloureteral units (PUUs) were selected at the Children's Hospital Affiliated to Zhejiang University School of Medicine from January 2021 to December 2024, 302 vesicoureteric reflux(VUR)-positive diagnosed by ceVUS was analyzed.IRR was defined as contrast agent infiltration into renal collecting tubules.Kidneys were divided into upper, middle, and lower thirds along the long axis for IRR localization.IRR detection rates across VUR grades and age groups were compared.Kendall’s correlation analysis was performed to evaluate spatial concordance between IRR and DMSA abnormalities in 98 patients(196 PUUs).
Results
The overall IRR detection rate was 20.86% (63/302 PUUs), exclusively observed in grade III-V VUR.Grade-specific detection rates were: III (27.08%, 26/96), IV (43.55%, 27/62), and V (52.63%,10/19).IRR incidence was significantly higher in infants<1 year (27.28% [35/126] vs 15.91% [28/176], P<0.05).IRR distribution was: upper (42.06%, 53/126)>lower (33.33%, 42/126)>middle (24.60%, 31/126).DMSA abnormalities occurred in 51.53% (101/196), showing a strong association with IRR (80.00% [44/55] vs 40.42%[57/141], P<0.05).DMSA abnormalities were distributed as: upper (47.78%, 75/157)>lower (36.94%, 58/157)>middle (15.29%, 24/157).IRR and DMSA abnormalities demonstrated a moderate spatial correlation (Kendall’s τ=0.543, P<0.05).
Conclusion
CeVUS effectively identifies IRR in grade III-V VUR, particularly in younger children.The spatial concordance between IRR and DMSA abnormalities supports incorporating IRR into VUR grading systems to optimize clinical decision-making.
表1 IRR 在肾脏的发生部位(个) |
| IRR 发生部位 | PUUs 计数 | 发生部位计数 |
|---|---|---|
| 上、中、下部 | 24 | 72 |
| 上部 | 17 | 17 |
| 下部 | 7 | 7 |
| 上、下部 | 8 | 16 |
| 上、中部 | 4 | 8 |
| 中、下部 | 3 | 6 |
| 合计 | 63 | 126 |
注:IRR 为肾内反流;PUUs 为肾盂-输尿管单位 |
| 1 |
Blumenthall.Vesicoureteric reflux and urinary tract infection in children[J].Postgrad Med J, 2006, 82(963): 31-35.
|
| 2 |
Brodeur AE, Goyer RA, Melick W.A potential hazard of barium cystography [J].Radiology, 1965, 85(6): 1080-1084.
|
| 3 |
Fukui S, Watanabe M, Yoshino K.Intrarenal reflux in primary vesicoureteral reflux[J].Int J Urol, 2013, 20(6): 631-636.
|
| 4 |
Cremin BJ.Observation on vesico-ureteric reflux and intrarenal reflux:a review and survey of material [J].Clin Radiol, 1979, 30(6): 607-621.
|
| 5 |
Gotoh T, Asano T, Nonomura K, et al.Intrarenal reflux in children with vesicouretetral reflux [J].Nihon Hinyokika Gakkai Zasshi, 1991,82(9): 1480-1486.
|
| 6 |
杨秀珍, 傅君芬, 叶菁菁, 等.排泄性尿路超声造影在儿童膀胱输尿管反流与尿道阴道疾病诊断中的应用[J].临床小儿外科杂志,2023, 22(10): 924-929.
|
| 7 |
Colleran GC, Paltiel HJ, Barnewolt CE, et al.Residual intravesical iodinated contrast: a potential cause of false-negative reflux study at contrast-enhanced voiding urosonography [J].Pediatr Radiol, 2016,46(11): 1614-1617.
|
| 8 |
Colleran GC, Paltiel HJ, Barnewolt CE, et al.Residual intravesical iodinated contrast: a potential cause of false-negative reflux study at contrast-enhanced voiding urosonography [J].Pediatr Radiol, 2016,46(11): 1614-1617.
|
| 9 |
Erica L, Klein Mary R, Wyers Francis MP, et al.Prevalence of intrarenal reflux in pediatric patients on contrastenhanced voiding urosonography [J].Pediatr Radiol, 2023, 53(3): 387-393.
|
| 10 |
Kim D, Choi YH, Choi G.Contrast-enhanced voiding urosonography for the diagnosis of vesicoureteral reflux and intrarenal reflux: a comparison of diagnostic performance with fluoroscopic voiding cystourethrography[J].Ultrasonography, 2021, 40: 530-537.
|
| 11 |
Majce AS, Arapovic A, Saraga-Babic M, et al.Intrarenal reflux in the light of contrast-enhanced voiding urosonography [J].Front Pediatr,2021, 9: 602477.
|
| 12 |
Faa G, Gerosa C, Fanni D, et al.Marked interindividual variability in renal maturation of preterm infants: lessons from autopsy [J].J Matern Fetal Neonatal Med, 2010, 23 Suppl 3: 129-133.
|
| 13 |
Hinchliffe SA, Sargent PH, Howard CV, et al.Human intrauterine renal growth expressed in absolute number of glomeruli assessed by dissector method and Cavalieri principle [J].Lab Invest, 1991, 64(6):777-784.
|
| 14 |
Tekgul S, Stein R, Bogaert G, et al.EAU-ESPU guidelines recommendations for daytime lower urinary tract conditions in children [J].Eur J Pediatr, 2020, 179(7): 1069-1077.
|
| 15 |
Ransley PG, Risdon RA.Renal papillary morphology and intrarenal reflux in the young pig[J].Urol Res, 1975, 3(3): 105-109.
|
| 16 |
Hodson CJ, Twohill SA.The time factor in the development of sterile renal scarring following high-pressure vesicoureteral reflux [J].Contrib Nephrol, 1984, 39: 358-369.
|
| 17 |
Simičić Majce A, Arapović A, Čapkun V, et al.The spectrum of pparenchymal changes in kidneys affected by intrarenal reflux,diagnosed by contrast-enhanced voiding urosonography and DMSA scan [J].Front Pediatr, 2022, 10: 886112.
|
| 18 |
Rushton HG, Majd M, Jonatansch B, et al.Renal scarring following reflux and nonreflux pyelonephritis in children: Enaluation with 99mTechnetium-dimercaptosuccinic acid scintigraphy[J].J Urol, 1992,147(5): 1327-1332.
|
| 19 |
Jacobsson B, Soderlundh S, Berg U.Diagnostic significance of 99mTc dimercaptosuccinic acid (DMSA) scintigraphy in urinary tract infection[J].Arch Dis Child, 1992, 67: 1338-1342.
|
| 20 |
Polito C, Rambaldi PF, Signorello G.Permanent renal parenchymal defects after febrile UTI are closely associated with vesicoureteral reflux[J].Pediatr Nephrol, 2006, 21: 521-526.
|
| 21 |
Saraga M, Saraga-Babić M, Arapović A, et al.The intrarenal reflux diagnosed by contrast-enhanced voiding urosonography (ceVUS):A reason for the reclassification of vesicoureteral reflux and new therapeutic approach? [J].Biomedicines, 2024, 12(5): 1015.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}