
2025 , Vol. 22 >Issue 03: 238 - 246
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.03.008
超声造影定量指标对初治原发性肝癌患者经皮微波消融术后复发的预测价值
Copy editor: 吴春凤
收稿日期: 2025-01-14
网络出版日期: 2025-06-10
基金资助
东方肝胆外科医院医工交叉研究项目(2022YGJ001)东方肝胆外科医院国家自然科学基金青年培养项目(2021GZR003)
版权
Predictive value of Vuebox indices derived from contrast-enhanced ultrasound for recurrence after percutaneous microwave coagulation therapy in patients with untreated primary hepatocellular carcinoma
Received date: 2025-01-14
Online published: 2025-06-10
Copyright
目的
探讨超声造影定量指标与初治原发性小肝癌患者经皮微波消融术(PMCT)术后复发的相关性。
方法
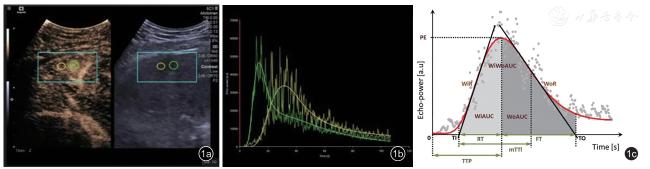
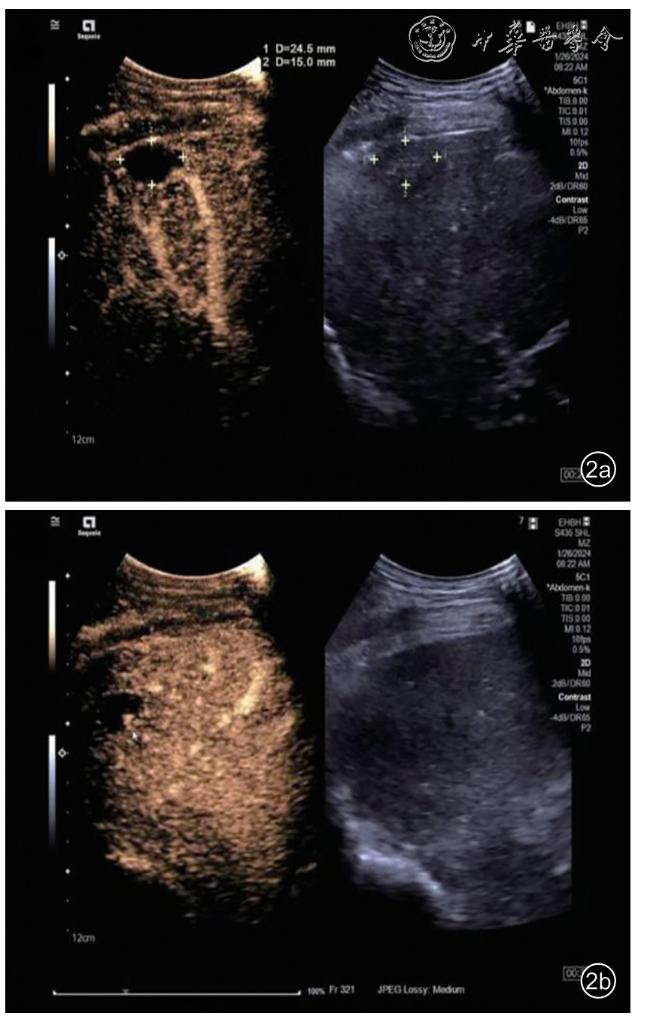
本研究为回顾性队列研究,选取海军军医大学第三附属医院东方肝胆外科医院自2022年6月至2023年11月间接收的277例初治原发性小肝癌患者作为研究对象。所有入选患者均在PMCT前接受血清学检验、超声造影及Vuebox量化分析。通过单因素和多因素Cox回归分析,探讨影响PMCT术后1年复发的危险因素。采用Kaplan-Meier生存曲线展示不同因素对复发的影响。
结果
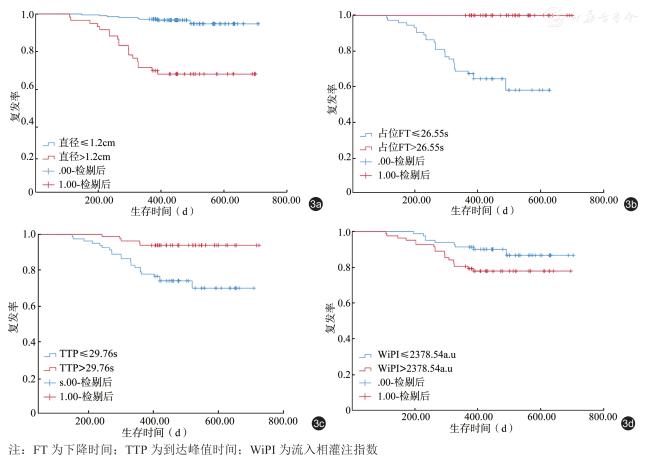
单因素Cox回归分析显示,肿瘤直径、高血压、术前甲胎蛋白、占位区平均线性度(MeanLin)、占位区上升时间(RT)、占位区平均渡越时间(mTTI)等因素具有统计学意义(P<0.05)。多因素Cox回归模型结果显示肿瘤直径(P<0.001)、占位区下降时间(FT,P=0.002)、肝组织到达峰值时间(TTP,P=0.014)、肝组织流入相灌注指数(WiPI,P=0.018)是局部肿瘤复发的独立影响因素。Kaplan-Meier曲线分析显示不同肿瘤直径(≤1.20 cm vs >1.20 cm)、占位区FT(>26.55 s vs ≤26.55 s)、肝组织TTP(>29.76 s vs ≤29.76 s)和肝组织WiPI(≤2378.54 a.u vs >2378.54 a.u)随访期间复发率分别为3.68% vs 31.67% 、0 vs 36.99%、6.10% vs 27.16%和11.11% vs 21.95%,进一步展示了这些因素对肿瘤复发具有预测价值(P<0.001、<0.001、<0.001、= 0.049)。
结论
超声造影定量指标中的定量参数占位FT、肝组织TTP、肝组织WiPI与小肝癌患者PMCT术后1年复发相关,对预测肝癌复发具有重要的临床参考价值。
顾怡君 , 李奕冉 , 钱艺 , 蒋栋 . 超声造影定量指标对初治原发性肝癌患者经皮微波消融术后复发的预测价值[J]. 中华医学超声杂志(电子版), 2025 , 22(03) : 238 -246 . DOI: 10.3877/cma.j.issn.1672-6448.2025.03.008
Objective
To investigate the correlation between quantitative indices derived from contrast-enhanced ultrasound (CEUS) and recurrence after percutaneous microwave coagulation therapy(PMCT) in patients with untreated primary hepatocellular carcinoma.
Methods
This is a retrospective cohort study, including 277 patients with primary small HCC who received initial treatment at Shanghai Eastern Hepatobiliary Surgery Hospital between June 2022 and November 2023. All enrolled patients underwent preoperative serum tests, CEUS, and quantitative analysis before PMCT treatment. Univariate and multivariate Cox regression analyses were performed to explore the risk factors for recurrence within one year after PMCT. Kaplan-Meier survival curves were used to demonstrate the impact of various factors on recurrence.
Results
In univariate Cox regression analysis, factors such as tumor diameter, hypertension,preoperative alpha-fetoprotein (AFP), lesion mean linearity (MeanLin), lesion rise time (RT), and lesion mean transit time showed statistical significance (P<0.05). The multivariate Cox regression model identified tumor diameter (P<0.001), lesion full time (FT) (P=0.002), hepatic tissue time to peak (TTP) (P=0.014), and hepatic tissue wash-in perfusion index (WiPI) (P=0.018) as significant predictors of local tumor recurrence. Kaplan-Meier curve analysis showed that tumor diameter (≤1.20 cm vs >1.20 cm), lesion FT (> 26.55 s vs ≤26.55 s),hepatic tissue TTP (> 29.76 s vs ≤29.76 s), and hepatic tissue WiPI (≤2378.54 a.u vs >2378.54 a.u) were significantly associated with recurrence rates during follow-up (3.68% vs 31.67%, 0 vs 36.99%, 6.10% vs 27.16%, and 11.11% vs 21.95%, respectively), further demonstrating the predictive value of these factors for tumor recurrence.
Conclusion
Quantitative parameters from contrast-enhanced ultrasound, including lesion FT, hepatic tissue TTP, and hepatic tissue WiPI, are associated with recurrence within one year after PMCT in patients with primary small HCC. The Vuebox quantitative parameters based on CEUS have important clinical application value in liver cancer recurrence prediction.
 表示,非正态分布的计量资料使用M(Q1,Q3)描述,计数资料采用频数(%)描述。采用单因素和多因素COX回归分析与PMCT术后1年复发相关的影响因素。对多因素Cox回归分析中有统计学意义的因素,绘制Kaplan-Meier曲线展示复发率之间的差异,并使用LogRank检验验证。P<0.05表示差异具有统计学意义。
表示,非正态分布的计量资料使用M(Q1,Q3)描述,计数资料采用频数(%)描述。采用单因素和多因素COX回归分析与PMCT术后1年复发相关的影响因素。对多因素Cox回归分析中有统计学意义的因素,绘制Kaplan-Meier曲线展示复发率之间的差异,并使用LogRank检验验证。P<0.05表示差异具有统计学意义。表1 227例超声引导下经皮微波消融治疗肝癌患者的基本临床资料 |
| 变量 | 数据 |
|---|---|
| 基本信息 | |
| 性别[ 例(%)] | |
| 男 | 171(61.73) |
| 女 | 106(38.26) |
| 年龄(岁, ± s ) | 59.18±11.86 |
| 体质量指数(kg/m2, ± s ) | 23.85±3.87 |
| 肿瘤直径(cm, ± s ) | 1.20±0.50 |
| 高血压[ 例(%)] | 86(31.04) |
| 糖尿病[ 例(%)] | 64(23.10) |
| 高血脂[ 例(%)] | 23(8.30) |
| 吸烟史[ 例(%)] | 82(29.60) |
| 饮酒史[ 例(%)] | 62(22.38) |
| 乙型肝炎病毒感染史[ 例(%)] | 220(79.42) |
| HBVDNA[ 例(%)] | 24(8.66) |
| 肝硬化[ 例(%)] | 234(84.48) |
| 门静脉高压[ 例(%)] | 18(6.50) |
| 术前实验室检查 | |
| 血小板(×109/L, ± s ) | 136.31±59.93 |
| 白细胞(×109/L, ± s ) | 5.02±1.79 |
| 血红蛋白(g/L, ± s ) | 138.28±19.09 |
| 中性粒细胞百分比(%, ± s ) | 60.45±38.70 |
| 淋巴细胞百分比(%, ± s ) | 31.54±18.87 |
| 凝血酶原时间(s, ± s ) | 12.01±1.16 |
| 部分凝血酶原时间(s, ± s ) | 28.45±2.34 |
| 凝血酶时间(s, ± s ) | 17.34±1.29 |
| 国际标准化比值( ± s ) | 1.00±0.11 |
| 总胆红素(μmol/L, ± s ) | 15.75±57.53 |
| 直接胆红素(μmol/L, ± s ) | 5.32±2.89 |
| 间接胆红素(μmol/L, ± s ) | 10.33±5.08 |
| 丙氨酸[μmol/L,M ( Q1, Q3 )] | 33.71(15.00,30.00) |
| 天门冬氨酸[μmol/L,M ( Q1, Q3 )] | 37.92(18.00,33.00) |
| 白蛋白(g/L, ± s ) | 41.25±4.72 |
| 前白蛋白(g/L, ± s ) | 197.48±64.67 |
| 异常凝血酶原[mAV/ml, M ( Q1, Q3 )] | 30.00(21.00,57.00) |
| 甲胎蛋白[ng/mL, M ( Q1, Q3 )] | 3.56(2.26,25.03) |
| 癌胚抗原[ng/mL, M ( Q1, Q3 )] | 2.46(1.71,3.66) |
| 癌抗原199 [U/ml, M ( Q1, Q3 )] | 10.60(6.10,19.80) |
| 超声造影定量指标[M ( Q1, Q3 )] | |
| 占位MeanLin(a.u) | 2356.79(1009.44,5217.58) |
| 占位PE(a.u) | 5468.53(2284.87,11951.49) |
| 占位WiAUC(a.u) | 41 465.93(15068.05,90089.66) |
| 占位RT(s) | 10.58(6.79,16.49) |
| 占位mTTI(s) | 59.13(36.51,132.31) |
| 占位TTP(s) | 14.11(9.92,19.32) |
| 占位WiR(a.u) | 807.17(357.51,1959.25) |
| 占位WiPI(a.u) | 3746.16(1495.71,7833.39) |
| 占位WoAUC(a.u) | 90 976.43(35827.87,208927.91) |
| 占位WiWoAUC(a.u) | 135 812.30(50307.64,297872.62) |
| 占位FT(s) | 26.55(14.63,42.93) |
| 占位WoR(a.u) | 231.67(74.24,591.34) |
| 占位Area(cm2) | 1.21(0.64,1.40) |
| 肝组织MeanLin(a.u) | 2201.35(1033.31,4207.85) |
| 肝组织PE(a.u) | 3446.68(1709.60,7937.00) |
| 肝组织WiAUC(a.u) | 63 898.34(26527.58,114685.30) |
| 肝组织RT(s) | 21.75(17.46,29.22) |
| 肝组织mTTI(s) | 128.80(54.50,343.14) |
| 肝组织TTP(s) | 29.76(23.30,37.86) |
| 肝组织WiR(a.u) | 333.85(110.83,591.68) |
| 肝组织WiPI(a.u) | 2 378.54(1216.25,5189.45) |
| 肝组织WoAUC(a.u) | 15 173.23(65553.57,295555.66) |
| 肝组织WiWoAUC(a.u) | 223 100.44(93437.29,422221.47) |
| 肝组织FT(s) | 48.23(36.32,65.35) |
| 肝组织WoR(a.u) | 100.43(44.89,214.67) |
| 肝组织Area(cm2) | 0.83(0.62,1.09) |
注:HBVDNA为乙型肝炎病毒脱氧核糖核酸;MeanLin为平均线性度;PE为峰值强度;WiAUC为流入相曲线下面积;RT为上升时间;mTTI为平均渡越时间;TTP为达峰值时间;WiR为流入相斜率;WiPI为流入相灌注指数;WoAUC为流出相曲线下面积;WiWoAUC为整体增强曲线下面积;FT为下降时间;WoR为流出相斜率;Area为病灶或肝组织面积 |
表2 超声引导下经皮微波消融治疗肝癌局部肿瘤术后1年复发的单因素Cox回归分析 |
| 因素 | B 值 | SE 值 | 瓦尔德值 | HR 值(95%CI) | P值 |
|---|---|---|---|---|---|
| 基本信息 | |||||
| 体质量指数 | -0.044 | 0.058 | 0.584 | 0.957(0.853 ~ 1.072) | 0.445 |
| 性别 | -0.608 | 0.439 | 1.914 | 0.545(0.230 ~ 1.288) | 0.167 |
| 年龄 | 0.013 | 0.017 | 0.623 | 1.013(0.981 ~ 1.047) | 0.430 |
| 肿瘤直径 | 1.737 | 0.239 | 53.051 | 5.682(3.560 ~ 9.069) | <0.001 |
| 高血压 | 0.769 | 0.385 | 3.982 | 2.158(1.014 ~ 4.592) | 0.046 |
| 糖尿病 | 0.380 | 0.422 | 0.812 | 1.462(0.640 ~ 3.340) | 0.368 |
| 高血脂 | -3.137 | 3.031 | 1.071 | 0.043(0.000 ~ 16.501) | 0.301 |
| 吸烟史 | 0.511 | 0.392 | 1.703 | 1.667(0.774 ~ 3.593) | 0.192 |
| 饮酒史 | 0.205 | 0.439 | 0.218 | 1.228(0.519 ~ 2.903) | 0.641 |
| 乙型肝炎病毒感染史 | 0.418 | 0.542 | 0.594 | 1.518(0.525 ~ 4.391) | 0.441 |
| HBVDNA | 0.638 | 0.542 | 1.386 | 1.893(0.654 ~ 5.478) | 0.239 |
| 肝硬化 | 0.396 | 0.612 | 0.418 | 1.486(0.447 ~ 4.935) | 0.518 |
| 门静脉高压 | -3.108 | 3.364 | 0.854 | 0.045(0.000 ~ 32.623) | 0.355 |
| 术前实验室检查 | |||||
| 血小板 | 0.000 | 0.004 | 0.019 | 1.000(0.994 ~ 1.007) | 0.891 |
| 白细胞 | 0.012 | 0.113 | 0.012 | 1.012(0.812 ~ 1.262) | 0.913 |
| 血红蛋白 | -0.013 | 0.010 | 1.693 | 0.988(0.969 ~ 1.006) | 0.193 |
| 中性粒细胞百分比 | 0.000 | 0.005 | 0.000 | 1.000(0.991 ~ 1.009) | 0.982 |
| 淋巴细胞百分比 | -0.019 | 0.021 | 0.851 | 0.981(0.942 ~ 1.022) | 0.356 |
| 凝血酶原时间 | 0.051 | 0.156 | 0.109 | 1.053(0.776 ~ 1.429) | 0.741 |
| 部分凝血酶原时间 | 0.054 | 0.078 | 0.480 | 1.055(0.906 ~ 1.229) | 0.488 |
| 凝血酶时间 | -0.146 | 0.155 | 0.890 | 0.864(0.637 ~ 1.171) | 0.346 |
| 国际标准化比值 | 0.459 | 1.621 | 0.080 | 1.583(0.066 ~ 37.966) | 0.777 |
| 总胆红素 | -0.025 | 0.032 | 0.624 | 0.975(0.916 ~ 1.038) | 0.430 |
| 直接胆红素 | -0.021 | 0.075 | 0.076 | 0.979(0.845 ~ 1.135) | 0.782 |
| 间接胆红素 | -0.046 | 0.049 | 0.870 | 0.955(0.867 ~ 1.052) | 0.351 |
| 丙氨酸 | -0.002 | 0.005 | 0.105 | 0.998(0.988 ~ 1.008) | 0.746 |
| 天门冬氨酸 | 0.003 | 0.003 | 0.996 | 1.003(0.997 ~ 1.010) | 0.318 |
| 白蛋白 | -0.007 | 0.044 | 0.026 | 0.993(0.910 ~ 1.083) | 0.871 |
| 前白蛋白 | -0.005 | 0.003 | 2.300 | 0.995(0.989 ~ 1.001) | 0.129 |
| 异常凝血酶原 | 0.000 | 0.001 | 0.364 | 1.000(0.998 ~ 1.001) | 0.546 |
| 甲胎蛋白 | 0.001 | 0.000 | 16.095 | 1.001(1.000 ~ 1.001) | <0.001 |
| 癌胚抗原 | -0.030 | 0.056 | 0.276 | 0.971(0.869 ~ 1.084) | 0.599 |
| 癌抗原199 | -0.004 | 0.008 | 0.323 | 0.996(0.980 ~ 1.011) | 0.570 |
| 超声造影定量指标 | |||||
| 占位MeanLin | 0.000 | 0.000 | 9.829 | 1.000(1.000 ~ 1.000) | 0.002 |
| 占位PE | 0.000 | 0.000 | 17.758 | 1.000(1.000 ~ 1.000) | 0.198 |
| 占位WiAUC | 0.000 | 0.000 | 1.660 | 1.000(1.000 ~ 1.000) | 0.198 |
| 占位RT | -0.388 | 0.079 | 24.249 | 0.679(0.582 ~ 0.792) | <0.001 |
| 占位mTTI | -0.018 | 0.007 | 6.843 | 0.982(0.969 ~ 0.996) | 0.009 |
| 占位TTP | -0.185 | 0.045 | 17.185 | 0.831(0.761 ~ 0.907) | <0.001 |
| 占位WiR | 0.000 | 0.000 | 27.339 | 1.000(1.000 ~ 1.000) | <0.001 |
| 占位WiPI | 0.000 | 0.000 | 16.987 | 1.000(1.000 ~ 1.000) | <0.001 |
| 占位WoAUC | 0.000 | 0.000 | 0.040 | 1.000(1.000 ~ 1.000) | 0.842 |
| 占位WiWoAUC | 0.000 | 0.000 | 0.289 | 1.000(1.000 ~ 1.000) | 0.591 |
| 占位FT | -0.155 | 0.033 | 22.250 | 0.856(0.803 ~ 0.913) | <0.001 |
| 占位WoR | 0.000 | 0.000 | 24.940 | 1.000(1.000 ~ 1.000) | <0.001 |
| 占位Area | -0.067 | 0.199 | 0.113 | 0.935(0.634 ~ 1.381) | 0.737 |
| 肝组织MeanLin | 0.000 | 0.000 | 3.732 | 1.000(1.000 ~ 1.000) | 0.053 |
| 肝组织PE | 0.000 | 0.000 | 6.599 | 1.000(1.000 ~ 1.000) | 0.010 |
| 肝组织WiAUC | 0.000 | 0.000 | 2.075 | 1.000(1.000 ~ 1.000) | 0.150 |
| 肝组织RT | -0.101 | 0.028 | 12.739 | 0.904(0.855 ~ 0.955) | <0.001 |
| 肝组织mTTI | -0.003 | 0.001 | 3.526 | 0.997(0.995 ~ 1.000) | 0.060 |
| 肝组织TTP | -0.077 | 0.021 | 13.831 | 0.926(0.890 ~ 0.964) | <0.001 |
| 肝组织WiR | 0.001 | 0.000 | 12.140 | 1.001(1.000 ~ 1.001) | <0.001 |
| 肝组织WiPI | 0.000 | 0.000 | 6.444 | 1.000(1.000 ~ 1.000) | 0.011 |
| 肝组织WoAUC | 0.000 | 0.000 | 1.970 | 1.000(1.000 ~ 1.000) | 0.160 |
| 肝组织WiWoAUC | 0.000 | 0.000 | 2.126 | 1.000(1.000 ~ 1.000) | 0.145 |
| 肝组织FT | -0.048 | 0.014 | 11.118 | 0.953(0.926 ~ 0.980) | 0.001 |
| 肝组织WoR | 0.002 | 0.001 | 14.107 | 1.002(1.001 ~ 1.003) | <0.001 |
| 肝组织Area | -0.046 | 0.499 | 0.008 | 0.955(0.359 ~ 2.538) | 0.927 |
注:HBVDNA为乙型肝炎病毒脱氧核糖核酸;MeanLin为平均线性度;PE为峰值强度;WiAUC为流入相曲线下面积;RT为上升时间;mTTI为平均渡越时间;TTP为到达峰值时间;WiR为流入相斜率;WiPI为流入相灌注指数;WoAUC为流出相曲线下面积;WiWoAUC为整体增强曲线下面积;FT为下降时间;WoR为流出相斜率;Area为病灶或肝组织面积 |
表3 超声引导下经皮微波消融治疗肝癌局部肿瘤复发的多因素Cox回归分析 |
| 因素 | B 值 | 标准误 | 瓦尔德值 | HR(95%CI)值 | P值 |
|---|---|---|---|---|---|
| 肿瘤直径 | 1.362 | 0.368 | 13.671 | 3.905(1.897 ~ 8.039) | <0.001 |
| 占位FT | -0.206 | 0.066 | 9.819 | 0.814(0.716 ~ 0.926) | 0.002 |
| 肝组织TTP | -0.082 | 0.033 | 6.093 | 0.921(0.863 ~ 0.983) | 0.014 |
| 肝组织WiPI | 0.000 | 0.000 | 5.583 | 1.000(1.000 ~ 1.000) | 0.018 |
注:HR为风险比;FT为下降时间;TTP为到达峰值时间;WiPI为流入相灌注指数 |
| 1 |
Huang GW, Tao YM, Ding X. Endocan expression correlated with poor survival in human hepatocellular carcinoma [J]. Dig Dis Sci,2009, 54(2): 389-394.
|
| 2 |
Lai EC, Lau WY. The continuing challenge of hepatic cancer in Asia [J].Surgeon, 2005, 3(3): 210-215.
|
| 3 |
Yang YF, Zhao W, Zhong YD, et al. Interferon therapy in chronic hepatitis B reduces progression to cirrhosis and hepatocellular carcinoma: a meta-analysis [J]. J Viral Hepat, 2009, 16(4): 265-271.
|
| 4 |
Lau WY, Lai EC. Hepatocellular carcinoma: Current management and recent advances [J]. Hepatobiliary Pancreat Dis Int, 2008, 7(3): 237-257.
|
| 5 |
汤钊猷. 汤钊猷临床肝癌学 [M]. 上海: 上海科技教育出版社,2001: 91.
|
| 6 |
Seki T, Wakabayashi M, Nakagawa T, et al. Ultrasonically guided percutaneous microwave coagulation therapy for small hepatocellular carcinoma [J]. Cancer, 1994, 74(3): 817-825.
|
| 7 |
Kosugi C, Furuse J, Ishii H, et al. Needle tract implantation of hepatocellular carcinoma and pancreatic carcinoma after ultrasoundguided percutaneous puncture: clinical and pathologic characteristics and the treatment of needle tract implantation [J]. World J Surg, 2004,28(1): 29-32.
|
| 8 |
Ohmoto K, Yoshioka N, Tomiyama Y, et al. Comparison of therapeutic effects between radiofrequency ablation and percutaneous microwave coagulation therapy for small hepatocellular carcinomas [J]. J Gastroenterol Hepatol, 2009, 24(2): 223-227.
|
| 9 |
Heisterkamp J, Hillegersberg L, Muider P, et al. Importance of eliminating portal flow to produce large intrahepatic lesions with interstit laser coagulation [J]. Br J Surg, 1997, 84(9): 1245-1248.
|
| 10 |
骆惊涛, 魏玺, 周洪渊, 等. 肝癌射频消融术后肝内远处复发的相关因素分析 [J]. 中华外科杂志, 2009, 47(20): 1529-1531.
|
| 11 |
Nylund K, Saevik F, Leh S, et al. Interobserver analysis of CEUS-derived perfusion in fibrotic and inflammatory Crohn’s disease [J].Ultraschall Med, 2019, 40(1): 76-84.
|
| 12 |
陈敏华. 杨蔽肝癌的射频治疗 [J]. 继续医学教育, 2006, 20(8): 103-108.
|
| 13 |
Dong BW, Liang P, Yu XL, et al. Sonographically guided microwave coagulation treatment ofliver cancer: 811 experimental and clinical study [J]. AJR, 1998, 171(2): 449-454.
|
| 14 |
Fan ST, Lo CM, Liu CL, et al. Hepatectomy for hepatocellular carcinoma: toward zero hospital deaths [J]. Ann Surg, 1999, 229(3):322-330.
|
| 15 |
Golberg SN, Grazelle GS, Halpem EF, et al. Radio-frequency tissue ablation importance of local temperature along the electrode tip exposure in determining lesion shape and size [J]. Acad Rmtio, 1996,3(3): 212-218.
|
| 16 |
Seki T, Wakabayashi M, Imamura M, et al. Percutaneous microwave coagulation therapy for patients with small hepatocellular carcinoma:comparison with percutaneous ethanol injection therapy [J]. Cancer,1999, 85(8): 1694-1702.
|
| 17 |
崔兆勋, 毛景涛, 李子良, 等. 经皮微波固化治疗小肝癌患者复发和预后的相关因素研究 [J]. 实用癌症杂志, 2015, 30(9): 1383-1385.
|
| 18 |
张镰竞. 胰腺癌超声造影Vuebox定量参数与病理分级的相关性分析 [D]. 吉林: 吉林大学, 2024: 2328.
|
| 19 |
苏荃利, 李玲玲, 邓芸霞, 等. 超声造影定性特征和VueBox定量参数评估乳腺癌分子分型的应用价值 [J]. 中华超声影像学杂志,2023, 32(5) : 399-405.
|
| 20 |
曹佳颖, 范培丽, 董怡, 等. 二维与三维超声造影定量分析技术评估肝肿瘤的对比研究 [J]. 中华超声影像学杂志, 2018, 27(5): 397-400.
|
| 21 |
肖雅丽, 李丛辉. 超声造影联合miR-599水平在原发性肝癌TACE预后评估中的价值 [J]. 中国医学物理学杂志, 2024, 41(4): 439-443.
|
| 22 |
王会哲, 卢双动, 王谦, 等. 超声参数联合肝动脉参数、C反应蛋白对肝癌介入治疗不良预后及复发预测价值 [J]. 转化医学杂志,2024, 13(7): 1021-1026.
|
| 23 |
Woo JC, Minseok S, Chul JP, et al. Radiation major hepatectomy using ablative dose yttrium-90 radioembolization in patients with large hepatocellular carcinoma 5 cm or larger [J]. J Vasc Interv Radiol,2023, 35(2): 203-212.
|
| 24 |
乔志重. 超声造影定量分析鉴别肝脏局灶性结节性增生与原发性肝癌初步探讨 [J]. 实用肝脏病杂志, 2019, 22(3): 421-424.
|
/
| 〈 |
|
〉 |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}