
2025 , Vol. 22 >Issue 06: 556 - 563
DOI: https://doi.org/10.3877/cma.j.issn.1672-6448.2025.06.009
母胎超声参数对复发性流产孕妇不良妊娠结局的预测价值
通信作者:
陈健,Email:chenjian9821@hotmail.comCopy editor: 汪荣
收稿日期: 2025-03-13
网络出版日期: 2025-08-01
基金资助
国家自然科学基金项目(82170301)
版权
Predictive value of maternal and fetal ultrasound parameters for adverse pregnancy outcomes in pregnant women with recurrent miscarriage
Corresponding author:
Chenjian, Email: chenjian9821@hotmail.comReceived date: 2025-03-13
Online published: 2025-08-01
Copyright
探讨复发性流产(RSA)孕妇孕中晚期母胎超声参数与妊娠结局的关系及超声参数评估不良妊娠结局(APO)的效能。
前瞻性选取2022年6月至2024年2月在深圳市第二人民医院生殖科于孕25~31周诊断为RSA的孕妇61例。超声监测母体双侧子宫动脉(UtA)血流参数[搏动指数(PI)、阻力指数(RI)],胎儿大脑中动脉(MCA)血流参数[收缩期峰值流速(PSV)、PI],胎儿脐动脉(UA)血流参数[收缩期峰值流速与舒张期末流速比值(S/D)、RI和PI];通过计算UtA-PI及UtA-RI的平均值,得出平均搏动指数(MPI)和平均阻力指数(MRI);根据公式计算脑胎盘比(CPR) [CPR=MCA-PI/UA-PI],同时监测腹内段脐静脉(IUV)及游离段脐静脉(FUV)内径(D)和时间平均峰值流速(TAmax);根据公式计算脐静脉血流量(UVBF) [Q=0.5 TAmax×π×(D/2)2]。随访妊娠结局,将61例孕妇分为正常妊娠结局组及APO组;分析母胎超声参数与APO的相关性及预测价值。
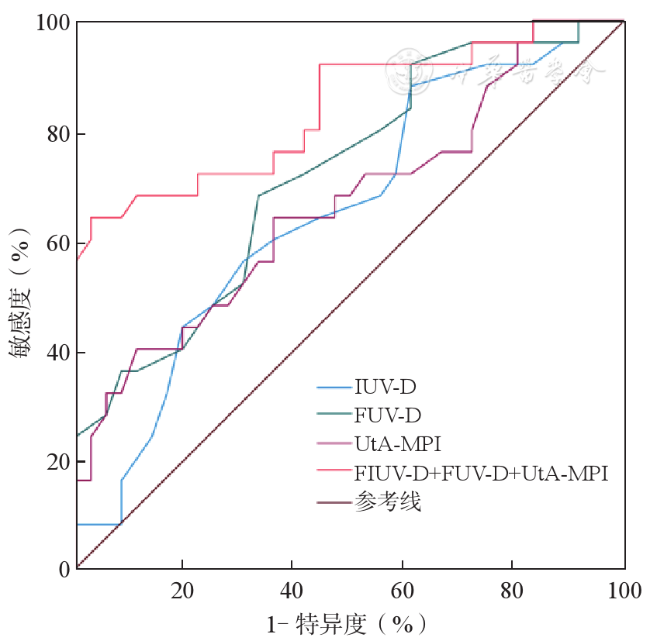
61例孕妇中,发生APO 25例。APO组孕妇UtA-MPI、UtA-MRI及胎儿IUV-D、FUV-D、游离段脐静脉血流量(FUVBF)均高于正常妊娠结局组,差异均有统计学意义[0.85±0.24 vs 0.71±0.16,0.53±0.09 vs 0.48±0.07,0.50(0.45,0.54)vs 0.47(0.43,0.51),0.63±0.07 vs 0.57±0.06,159.92±48.38 vs 131.41±38.40;P均<0.05]。Lasso回归分析结果显示,IUV-D、FUV-D、UtA-MPI为与APO相关的预测因子。上述3项指标预测APO的ROC曲线下面积分别为0.653、0.718、0.666,3项指标联合预测的ROC曲线下面积为0.839(95%CI:0.732~0.946),敏感度为64.0%,特异度为97.2%。
RSA孕妇在妊娠25~31周时的孕妇UtA-MPI、UtA-MRI及胎儿IUV-D、FUV-D、FUVBF与妊娠结局有关。IUV-D、FUV-D及UtA-MPI可作为预测APO的重要指标,联合预测具有较好的预测效能,对指导高危妊娠具有一定的临床价值。
汪浪 , 何怡华 , 李征毅 , 刘翠云 , 颉剑锋 , 陈健 . 母胎超声参数对复发性流产孕妇不良妊娠结局的预测价值[J]. 中华医学超声杂志(电子版), 2025 , 22(06) : 556 -563 . DOI: 10.3877/cma.j.issn.1672-6448.2025.06.009
To investigate the relationship between maternal and fetal ultrasound parameters and pregnancy outcomes in pregnant women with a history of recurrent miscarriage (RSA) in the second and third trimesters of pregnancy and their efficacy in assessing the occurrence of adverse pregnancy outcomes (APOs).
From June 2022 to February 2024, we prospectively selected 61 pregnant women diagnosed with RSA who were seen at 25-31 weeks of pregnancy in the Department of Reproductive Medicine of Shenzhen Second People’s Hospital. We measured the pulsatility index (PI) and resistance index (RI) of the maternal bilateral uterine artery (UtA) and monitored the peak systolic flow velocity (PSV) and pulsatility index (PI) of the fetal middle cerebral artery (MCA) as well as the peak-systolic-velocity/end-diastolic-velocity (S/D) ratio, resistance index (RI), and PI of the fetal umbilical artery (UA). The mean pulsatility index (MPI) and mean resistance index (MRI) were derived by calculating the mean values of the UtA-PI and UtA-RI. We calculated the cerebroplacental ratio (CPR) according to the formula [CPR=MCA-PI/UA-PI]. We simultaneously measured the diameter (D) and time-averaged peak flow rate (TAmax) of the intra-abdominal umbilical vein (IUV) and the free loop of the umbilical vein (FUV), and calculated the umbilical vein blood flow (UVBF) according to the formula [Q=0.5TAmax×π×(D/2)2]. Pregnancy outcomes were followed, and the women were divided into either a normal pregnancy outcome group or an APO group. The correlation of maternal-fetal ultrasound parameters with APO was analysed, and their predictive value for APO was assessed.
Among the 61 pregnant women, 25 had APO. At 25-31 weeks of pregnancy, there were no statistically significant differences in fetal MCA-PSV, MCA-PI, UA-S/D ratio, UA-PI, UA-RI, IUV-TAmax, intra-abdominal umbilical vein blood flow (IUVBF), or FUV-TAmax between the two groups (P>0.05). Maternal UtA-MPI and UtA-MRI, as well as fetal IUV-D, FUV-D and FUVBF, were significantly higher in women with APO compared to those with normal pregnancy outcomes (0.85±0.24 vs 0.71±0.16, 0.53±0.09 vs 0.48±0.07, 0.50 [0.45, 0.54] vs 0.47 [0.43, 0.51], 0.63±0.07 vs 0.57±0.06, and 159.92±48.38 vs 131.41±38.40, respectively; P<0.05). Lasso regression was employed to identify three predictors of APO, which were IUV-D, FUV-D, and UtA-MPI. The AUC for the above three indexes to predict APO was 0.653, 0.718, and 0.666, respectively; the AUC of their combination was 0.839, with a sensitivity of 64.0% and specificity of 97.2%.
Maternal UtA-MPI and UtA-MPI, as well as fetal IUV-D, FUV-D, and FUVBF at 25-31 weeks of gestation in patients with RSA are associated with pregnancy outcomes. IUV-D, FUV-D, and UtA-MPI are important predictors of APO, and the combination of them has better predictive efficacy, which is clinically valuable in guiding high-risk pregnancies.
 ±s描述,组间比较采用独立样本t检验;非正态分布的采用M(Q1,Q3)描述,组间比较采用Mann-Whitney U检验。计数资料以例(%)表示,组间比较采用χ2检验或Fisher精确检验。采用Lasso逻辑回归法筛选与APO最相关的预测因子。绘制ROC曲线,并计算ROC曲线下面积(area under the curve,AUC)值检验预测因子的效能。以P<0.05为差异有统计学意义。
±s描述,组间比较采用独立样本t检验;非正态分布的采用M(Q1,Q3)描述,组间比较采用Mann-Whitney U检验。计数资料以例(%)表示,组间比较采用χ2检验或Fisher精确检验。采用Lasso逻辑回归法筛选与APO最相关的预测因子。绘制ROC曲线,并计算ROC曲线下面积(area under the curve,AUC)值检验预测因子的效能。以P<0.05为差异有统计学意义。表1 不良妊娠结局组与正常妊娠结局组RSA患者基线资料比较 |
| 临床资料 | 正常妊娠结局组(n=36) | APO组(n=25) | 统计值 | P值 |
|---|---|---|---|---|
年龄(岁, ±s) ±s) | 31.50±3.70 | 32.32±3.51 | t =0.87 | 0.388 |
孕前BMI(kg/m2, ±s) ±s) | 21.32±2.43 | 20.32±2.39 | t = -1.60 | 0.115 |
| 自然受孕[例(%)] | 28(77.8) | 21(84.0) | χ2 = 0.08 | 0.784 |
| 孕次[次,M(Q1,Q3)] | 3(3,4) | 4(3,5) | Z = -0.71 | 0.479 |
| 产次[次,M(Q1,Q3)] | 0(0,1) | 0(0,1) | Z = -0.77 | 0.444 |
检查孕周(周, ±s) ±s) | 28.02±1.70 | 28.65±1.64 | t = 1.43 | 0.157 |
| 抗心磷脂抗体阳性[例(%)] | 16(44.4) | 8(32.0) | χ2 = 0.96 | 0.328 |
| 抗β糖蛋白抗体阳性[例(%)] | 19(52.8) | 9(36.0) | χ2 = 1.67 | 0.196 |
| 抗核抗体阳性[例(%)] | 25(69.4) | 18(72.0) | χ2 = 0.05 | 0.830 |
| 抗SSA抗体阳性[例(%)] | 7(19.4) | 8(32.0) | χ2 = 1.25 | 0.263 |
| 抗SSB抗体阳性[例(%)] | 3(8.3) | 5(20.0) | χ2 = 0.89 | 0.346 |
| 抗Ro52抗体阳性[例(%)] | 12(33.3) | 13(52.0) | χ2 = 2.13 | 0.145 |
| 狼疮抗凝剂[例(%)] | 4(11.1) | 3(12.0) | χ2 = 0.00 | 1.000 |
| 肝素[例(%)] | 36(100) | 24(96.0) | - | 0.410 |
| 阿司匹林[例(%)] | 33(91.7) | 21(84.0) | χ2 = 0.27 | 0.606 |
| 羟氯喹[例(%)] | 31(86.1) | 23(92.0) | χ2 = 0.09 | 0.763 |
| 糖皮质激素[例(%)] | 27(75.0) | 22(88.0) | χ2 = 0.86 | 0.353 |
| 环孢素[例(%)] | 20(55.6) | 15(60.0) | χ2 = 0.12 | 0.730 |
注:APO为不良妊娠结局;RSA为复发性流产;BMI为体质量指数;-表示无数据 |
表2 不良妊娠结局组与正常妊娠结局组RSA患者子宫动脉相关血流参数比较( |
| 血流参数 | 正常妊娠结局组(n=36) | APO组(n=25) | t值 | P值 |
|---|---|---|---|---|
| MPI | 0.71±0.16 | 0.85±0.24 | 2.49 | 0.017 |
| MRI | 0.48±0.07 | 0.53±0.09 | 2.17 | 0.034 |
注:APO为不良妊娠结局;RSA为复发性流产;MPI为平均搏动指数;MRI为平均阻力指数 |
表3 不良妊娠结局组与正常妊娠结局组RSA患者的胎儿大脑中动脉相关血流参数比较( |
| 血流参数 | 正常妊娠结局组(n=36) | APO组(n=25) | t值 | P值 |
|---|---|---|---|---|
| PSV(cm/s) | 37.35±6.82 | 38.69±5.41 | 0.82 | 0.413 |
| PI | 1.93±0.42 | 1.92±0.35 | -0.11 | 0.915 |
| CPR | 1.93±0.50 | 1.96±0.46 | 0.25 | 0.801 |
注:APO为不良妊娠结局;RSA为复发性流产;PSV为收缩期峰值速度;PI为搏动指数;CPR为脑胎盘比 |
表4 不良妊娠结局组与正常妊娠结局组RSA患者的胎儿脐动脉相关血流参数比较( |
| 血流参数 | 正常妊娠结局组(n=36) | APO组(n=25) | t值 | P值 |
|---|---|---|---|---|
| S/D | 2.88±0.45 | 2.88±0.56 | -0.00 | 0.997 |
| PI | 1.02±0.15 | 1.01±0.18 | -0.39 | 0.701 |
| RI | 0.65±0.06 | 0.64±0.06 | -0.45 | 0.656 |
注:APO为不良妊娠结局;RSA为复发性流产;S/D为收缩期峰值流速与舒张期末流速比值;PI为搏动指数;RI为阻力指数 |
表5 不良妊娠结局组与正常妊娠结局组RSA患者的胎儿脐静脉相关血流参数比较 |
| 血流参数 | 正常妊娠结局组(n=36) | APO组(n=25) | 统计值 | P值 |
|---|---|---|---|---|
| IUV-D[cm,M(Q1,Q3)] | 0.47(0.43,0.51) | 0.50(0.45,0.54) | Z =-2.03 | 0.043 |
IUV-TAmax(cm/min, ±s) ±s) | 1363.15±329.71 | 1330.37±224.84 | t =-0.46 | 0.646 |
| IUVBF[ml/min,M(Q1,Q3)] | 114.00(78.62,153.12) | 132.21(101.49,169.38) | Z =-1.31 | 0.192 |
FUV-D(cm, ±s) ±s) | 0.57±0.06 | 0.63±0.07 | t =3.35 | 0.001 |
| FUV-TAmax[cm/min,M(Q1,Q3)] | 985.20(905.40,1083.90) | 1024.80(865.80,1108.50) | Z =-0.32 | 0.753 |
FUVBF(ml/min, ±s) ±s) | 131.41±38.40 | 159.92±48.38 | t =2.56 | 0.013 |
注:APO为不良妊娠结局;RSA为复发性流产;IUV为腹内段脐静脉;FUV为游离段脐静脉;D为内径;TAmax为时间平均峰值流速;IUVBF为腹内段脐静脉血流量;FUVBF为游离段脐静脉血流量 |
图1 Lasso系数路径图与回归分析交叉验证曲线。图a为Lasso系数路径图(上横坐标表示模型中非零系数的个数,下横坐标表示标准化后的系数向量log(λ),纵坐标是回归系数的值,垂直线对应于通过10倍交叉验证和拟合所选择的非零特征);图b为Lasso回归分析交叉验证曲线(纵坐标为交叉验证的误差,上横坐标为不同λ值对应的变量数,下横坐标为lambda惩罚系数的对数log(λ),模型采用10倍交叉验证方法,通过调整λ的不同参数,使模型的二项偏差最小,从而筛选出具有较高诊断价值的指标)。图中左侧虚线对应的参数(lambda. min)表示最小均方误差时的λ值,对应的变量数为4个;右侧虚线对应的参数(lambda.1se)代表最小λ右侧的1个标准误时的λ值,对应的变量数为3个 |
图2 IUV-D、FUV-D、UtA-MPI预测不良妊娠结局的ROC曲线注:IUV-D为腹内段脐静脉内径;FUV-D为游离段脐静脉内径;UtA-MPI为子宫动脉平均搏动指数 |
表6 孕中晚期脐静脉、子宫动脉超声参数对RSA孕妇APO的预测价值 |
| 诊断指标 | AUC | 标准误 | P值 | 95%CI | 敏感度(%) | 特异度(%) |
|---|---|---|---|---|---|---|
| IUV-D | 0.653 | 0.071 | 0.043 | 0.514~0.793 | 88.0 | 38.9 |
| FUV-D | 0.718 | 0.066 | 0.004 | 0.588~0.847 | 68.0 | 66.7 |
| UtA-MPI | 0.666 | 0.072 | 0.028 | 0.525~0.807 | 40.0 | 88.9 |
| IUV-D+FUV-D+UtA-MPI | 0.839 | 0.055 | <0.001 | 0.732~0.946 | 64.0 | 97.2 |
注:RSA为复发性流产;APO为不良妊娠结局;IUV-D为腹内段脐静脉内径;FUV-D为游离段脐静脉内径;UtA-MPI为子宫动脉平均搏动指数 |
汪浪,何怡华,李征毅,等.母胎超声参数对复发性流产孕妇不良妊娠结局的预测价值[J/OL].中华医学超声杂志(电子版), 2025, 22(6): 556-563.
| 1 |
中华医学会妇产科学分会产科学组,复发性流产诊治专家共识编写组. 复发性流产诊治专家共识(2022)[J]. 中华妇产科杂志, 2022, 57(9): 653-667.
|
| 2 |
|
| 3 |
范东晨, 李小花, 刘阿庆, 等. 彩色多普勒超声检测子宫动脉及螺旋动脉血流对复发性流产发生及围产期结局的预测价值[J]. 中国计划生育和妇产科, 2021, 13(11): 83-86.
|
| 4 |
|
| 5 |
|
| 6 |
郭娟, 韩建成, 谷孝艳, 等. 先天性心脏病胎儿与正常胎儿脐静脉血流量的对比研究[J]. 中华超声影像学杂志, 2022, 31(9): 774-778.
|
| 7 |
|
| 8 |
|
| 9 |
|
| 10 |
|
| 11 |
陈清爽, 苏新辉, 冉静, 等. 不同病因的复发性流产患者妊娠期子宫动脉血流变化及其临床意义[J]. 中国现代医药杂志, 2021, 23(10): 16-21.
|
| 12 |
|
| 13 |
|
| 14 |
|
| 15 |
|
| 16 |
侯留杰, 栗河舟, 张红彬, 等. 超声对晚发型胎儿生长受限不良围产期结局的预测价值[J/OL]. 中华医学超声杂志(电子版), 2022, 19(11): 1187-1192.
|
| 17 |
|
| 18 |
|
| 19 |
施如勇, 金平安, 陆晓东, 等. 胎儿脐动脉S/D比值及超声生长参数Z-评分评估妊娠期糖尿病孕妇胎儿生长受限的价值[J/OL]. 中华医学超声杂志(电子版), 2022, 19(6): 567-572.
|
| 20 |
|
| 21 |
|
| 22 |
李天刚, 车岩, 童明辉, 等. 静脉导管血流检测对妊娠高血压疾病胎儿右心舒张功能的评价[J]. 临床超声医学杂志, 2013, 15(2): 87-90.
|
| 23 |
|
| 24 |
|
| 25 |
|
| 26 |
|
| 27 |
|
| 28 |
|
/
| 〈 |
|
〉 |
 ±s)
±s) ±s)
±s) ±s)
±s)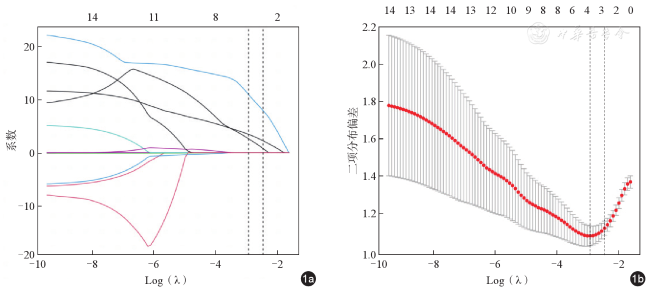
{kind=link}
{kind=link}
{kind=link}
{kind=link}